|
|
Alimentary
tract and pancreas Alimentarni
trakt i pankreas |
|
1Saša
Grgov, 1Perica
Stamenkovi}, 2Miroslav
Stefanovi} 1Gastroenterology Unit, 2Department of Pathology, Health Center of Leskovac, Serbia. |
ARCH
GASTROENTEROHEPATOL 2003; 22 (No 1 - 2): 12 – 17 Images
in clinical gastroenterology Endoloop-assisted
resection of
large gastric polyp Resekcija
velikog gastricnog polipa uz pomo} "endoloop-a" (
accepted April 24th 2003 ) |
|
|
Sixty-year
old patient was admitted for further evaluation of
his functional dyspepsia which manifested with chronic
epigastric pain, nausea, and occasional vomiting. His
was otherwise well noursihed gentleman enjoying good
health. His clinical findings was normal. All laboratory investigations
including: ESR, hematologic examination, urinalysis,
BUN, serum creatinine, blood sugar, AST,ALT,GGT,
alkaline phosphatase, total serum proteins, serum
albumin, PT,PTT time were all normal or negative. Upper
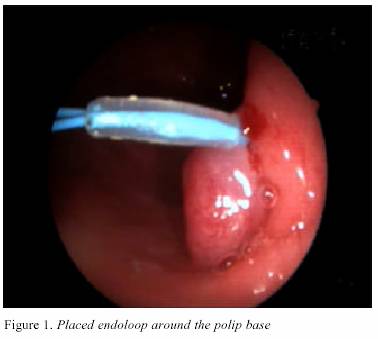
gastrointestinal (GI) endoscopy revealed near pyloric
ring,on the posterior wall of gastric antrum pedunculated polyp
20 mm in diameter. His pedicle was 30mm in
lenght and 10mm in diameter. Endoloop
aplicator with placed throught the working channel
of the scope and Olympus endoloop (40mm in diameter)
was fixed on the pedicle of the polyp which became
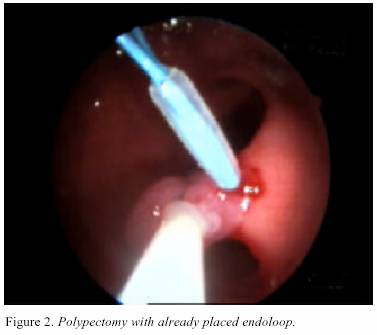
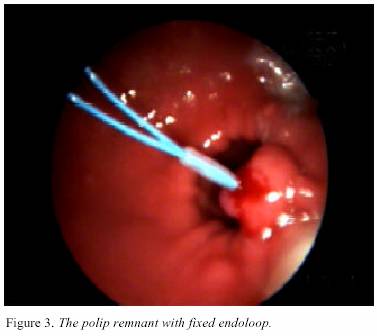
livid in coulor. Figure 1. Further on electroresection of
the polyp was performed with polyp retriveal by means
of endobasket. Endoloop was left in situ around the remnant
of polyp pedicle without residual bleeding Figure 2,3.
The patients was discharged next day. Twelve days later
follow-up upper GI endoscopy demonstrated completely normal
findings. There were no residual postpolypectmy changes
including the endolooped pedicle remnant. Histology
of the polyp was: the resceted polyp was brought
to the pathologist in toto. This was gastric hyperplastic polyp
with normal basis and clear-cut resection margin
towards the gastric wall. Comment:
This is further to demonstrate the usefulness of
two step approach to the resection of large GI polyps which
may possibly bleed after polypectomy. Pre-resectional endoloop
placement around the polyp pedicle may prevent
postpolypectomy bleeding and obviate endoscopic hemosatic
procedures or open surery. It seems that in selected
cases this endoscopic approach to the large GI polyps
is simple,safe, and cost-effective. This imply the necessity
for further improvements in GI endoscopic programmes for
trainees.
|
|
|