|
|
Alimentary
tract and pancreas Alimentarni
trakt i pankreas |
||
|
Vojislav N. Peri{i}, Mira Petrovi}, Dragana @ivanovi} University Childrení Hospital, Belgrade, Serbia. |
ARCH
GASTROENTEROHEPATOL 2003; 22 (No 1 - 2): 12 – 17 Case
report Duplex
ventral pancreas: another
cause of pancreatitis
in children Prikaz
slu~aja Dvostruki
vetralni pankreas: jo{ jedan uzrok pankreatitisa
u dece (accepted
April 4th, 2003) |
||
|
Key Words: ventral pancreas, duplication, pancreatitis, child. |
Abstract Duplication
of the ventral pancreatic ductal system was diagnosed in 4.5-year old boy
during his evaluation
for recurrent attacks of pancreatitis. Endoscopic retrograde
cholangiopancreatography demonstrated
typical changes of chronic pancreatitis confined to one ductal system, with
the other ductal
system was completely normal. Both ductal system opacified via commmon
opening at the vestibulum
of the major papilla. A minor papilla was present. This rare anomaly of the
ventral pancreas may
be another developmental cause of pancreatitis in children. Sa`etak Dvostruki
duktalni sistem ventralnog pankreasa je utvrdjen u 4.5-godinjeg deaka tokom
ispitivanja etiologije
ponavljanih napada akutnog pankreatitisa. Endoskopska retrogradna
holangiopankreatografija je
pokazala tipine promene za hronini pankreatitis ograniene na jedan duktalni sistem,
dok je drugi duktalni sistem bio potpuno normalan. Papila minor je bila
prisutna. Ova retka anomalija
mo`e da bude jo jedna razvojna abnormalnost odgovorna za pankreatitis u dece. |
||
|
Kljucne reci: funkcionalna dispepsija, podgrupe, Helicobacter pylori. |
|||
|
|
The
pancreas begins as two separate outpouchings arising from
oposite side of the caudal portion of the foregut in a
3-4week-old embryo (1). The dorsal primordium is to first
to arise from the posterior duodenal wall (2). The ventral pancreatic
component begins as diverticulum from the base
of the ventrally positioned hepatic diverticulum (2). This
portion of the pancreas usually develop a bifid structure with
a right and left ventral pancreatic lobe (bilobed embryonal
ventral pancreas) (1,2). Further on, the ventral pancreatic
segment usually becomes singular, whether by fusion
of these lobes or by atrophy of the left lobe (1,2,3). Then,
the ventral anlage undergoes clockwise rotation to rest
just inferior and posterior to the dorsal pancreatic segment. Fusion
of dorsal and ventral pancreatic primordium at
7-8 weks of embryonic life result in a mature pancreas (4).
If the 2 pancreatic primordium and their ductal system do
not fuse, the congenital anomaly of pancreas divisum results
(1,2,4,5). The
anomaly of duplex ventral pancreas is when both left
and lateral ventral pancreatic lobes ductal systems persists after
clockwise rotation and fusion of one of them with
dorsal pancreas. Here
we report the paediatric case of duplex ventral pancreas
presented as recurrent pancreatitis. CASE
REPORT A
4.5-year old boy has been suffering of seven attacks of acute
pancreatitis for about 1.5 year. His clinical findings was
unremarcable. Laboratory investigations revealed elevated
serum and urinary amylase level, 1580 and 4320 IU/L
respectivelly. Serum electrolytes, lipid profile, sweat chloride
concentration, stool examination for ova and parasites were
either normal or negative. An abdominal ultrasound scan
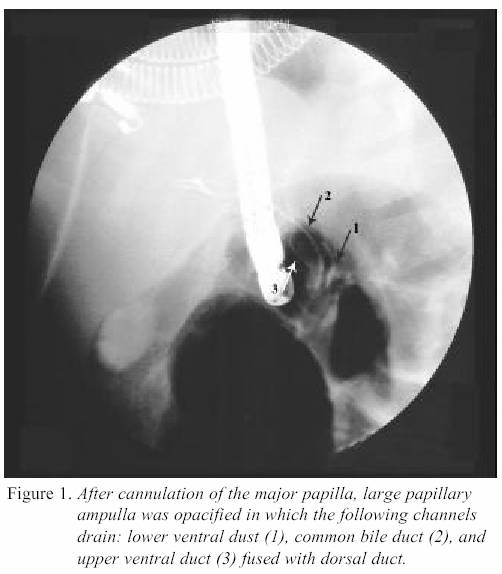
was normal. Endoscopic retrograde cholangiopancreatography (ERCP)
showed complete duplication of
ductal system. Both ductal systems filled by injection of contrast
material through the major papilla into the large papillary
ampulla. Figure 2. The upper ductal system appeared
normal. The lower ductal system was sligtly dilated
with irregular caliber. The patient is treated conservatively with
omeprazole 20mg/daily, pancreatic enzyme supplementation
and dieting. A six months follow up showed
two mild flares of pancreatitis.
DISCUSSION During
embryological development, the ventral pancreatic primordium
has complicated route of transformation (6).
This portion of pancreas usually develop bifid (bilobated) appearance
with a right and left ventral lobe. Although
this initial structure may become important in the
production of the annular pancreas, the ventral pancreatic segment
usually become singular, either by fusion of these
lobes or by atrophy of the left lobe. If the fusion doesdraining
the entire gland via the major papilla. A
review of the literature regarding pancreatic ductal variation
of the ventral pancreas has revealed one reference to
the anomaly of the ventral pancreas in two adult patients reported
by Agha (7). Both cases suffered of recurrent pancreatitis. As
in our paediatric patient, in both adult cases of Agha
only one ductal system was diseased (7). This lead us to
speculate that this ductal anomaly may predispose do pancreatitis. |
||
|
|
REFERENCES: 1.
Taylor AJ, Bohorfoush
AG. Interpretation of ERCP. Philadelphia:Lipincott, 1997. 2.
Belber JP, Bill K.
Fison anomalies of the pancreatic ductal system: differentiation from
pathologic states. Radiology 1977; 123:637-42. 3.
Glazer GM, Margulis AR.
Annular pancreas: etiology and diagnosis usind endoscopic
retrograde cholangiopancratography. Radiology
1979; 133:303-8. |
4.
Delhaye M, Engelholm L,
Cremer M. Pancreas divisum: congenital anatomic variant or
anomaly? Contribution of endoscopic retrograde
dorsal pancreatography. Gastroenterology 1985; 89:951-8. 5.
Cotton PB. Congenital
anomaly of pancreas divisum as cause of obstructive pain and
pancreatitis. Gut 1980; 21:105-14. 6.
Freeny PC, Lawson TL.
Embryology of the pancreas and biliary tract. In: Freeny PC,
Lawson TL, eds. Radiology of the pancreas. New York:Springer Verlag, 1982;pp 98-144. |
7.
Agha FP. Duplex ventral
pancreas. Gastrointest Radiol 1987; 12:23-5. |