|
|
Alimentary
tract and pancreas Alimentarni
trakt i pankreas |
||
|
1Yasar Nazligul, 2Muharrem Btirenen, 1H. Ilyas Ozardali, 3Mustafa Ulukanligil, 1Bülent Tumkaya Departments of 1Internal Medicine, 2Pathology2 and 3Microbiology, Harran University Medical Faculty, Sanliurfa, Turkey. |
ARCH
GASTROENTEROHEPATOL 2003; 22 (No 1 - 2): 12 – 17 Helicobacter
pylori infection in
dyspepsia subgroups in one
region of Turkey Infekcija
Helicobacter-om pylori u podgrupama dispepsija
u jednom regionu Turske (accepted
April 6th 2003 ) |
||
|
Key Words: Functional dyspepsia, subgroups, Helicobacter pylori. |
Abstract Purpose:
Different subgroups exist among patients with functional
dyspepsia (FD) based on predominant symptoms.
The aetiopathogenesis of symptoms is still unclear; however, Helicobacter pylori
(H. pylori)
and several other factors have been implicated. We investigated H.
pylori prevalence in
FD subgroups and compared with non-dyspeptic controls. Methods:
The study carried out on 174 patients with FD and 17
non-dyspeptic subjects, which underwent
upper gastrointestinal endoscopy. H. pylori identification
was done by histology using biopsy
samples taken from antral mucosa. Results:
H. pylori was identified in 86 of
111 (77.5%) patients in ulcer like subgroup, 22 of 36 (61.1%)
patients in dysmotility like subgroup, in 19 of 27 (70.4%) patients in
unspecified subgroup, in
12 of 17 (70.6%) in controls. H. pylori prevalence
in patients with ulcer like dyspepsia was higher than
other subgroups and controls, but differences were not statistically
significant. Conclusion:
Our data imply that Helicobacter pylori infection
has not an important influence on symptoms
in patients with functional dyspepsia. Sazetak Cilj:
Medju
pacijentima sa funkcionalnom dispepsijom (FD) postoji vi{e razli~itih
podgrupa koje su formirane
na osnovu preovladjuju}ih simptoma. Etiopatogenetski uzrok tegoba nije u
potpunosti jasan.
Medjutim medju ostalim ~iniocima ~ini se da Helicobacter
pylori (HP) ima zna~ajnu ulogu. U ovoj
studiji na{ cilj je bio da ispitamo prevalenciju HP
u
podgrupama FD te da dobijene rezultate uporedimo
sa kontrolnom nedispepti~kom grupom. Metode:
Ova
studija je obuhvatila 174 pacijenta sa FD i 17 osoba nedispepti~kim tegobama
koje su iz
drugih razloga bile podvrgnute proksimalnoj digestivnoj endoskopiji.
Identifikacija HP je na~injena na
osnovu histolo{kih pregleda uzoraka antralne sluznice. Rezultati:
HP
je
bio otkriven u 86 od 111 (77.5%) pacijenata sa dispepsijom ulkusnog tipa, 22
od 36
pacijenata (61.1%) sa dispepsijom tipa dismotiliteta, i u 19 od 27 osoba
(70.4%) sa nespecificiranom FD. U
kontrolnoj grupi 12 od 17 (70.6%) je bilo HP pozitivno.
U ispitanika sa FD ulkusnog tipa
prevalencija HP je bila vi{a nego u drugim podgrupama
FD, medjutim razlika nije bila statisti~ki signifikantna. Zakljucak:
Rezultati
na{eg ispitivanja ukazuju da infekcija sa HP nije od
presudnog zna~aja na simptome
pacijenata sa FD. |
||
|
Kljucne
reci: funkcionalna
dispepsija, podgrupe, Helicobacter
pylori. |
|||
|
|
INTRODUCTION Dyspepsia has been defined as chronic or recurrent
epigastric pain or upper abdominal discomfort whith accompanied symptoms such as nausea, early satiety, postprandial fullness or bloating. Approximately half of all patients with dyspepsia do not have definite structural or laboratory explanation for their symptoms, and are labeled as having functional dyspepsia (FD). The patients with FD are subcategorized according to predominant symptoms into ulcer like dyspepsia, dysmotility like dyspepsia and unspecified dyspepsia (1-4). The etiopathogenesis of FD is unclear; however, it has been implicated various factors such as motility disorders, gastric acid, visceral hypersensitivity, central nervous
system dysfunction, psychological factors, and H. pylori infection (4-7). The aim of the present clinical study was to investigate H. pylori prevalence
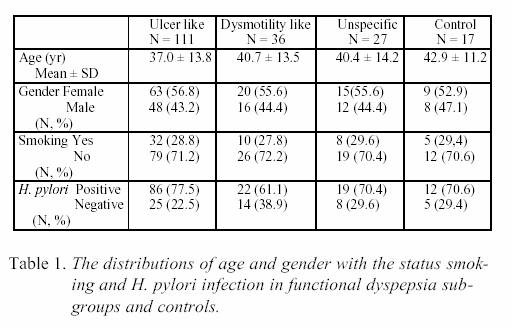
in FD subgroups and to compare with non-dyspeptic subjects. PATIENTS AND METHODS One hundred seventy four patients (98 female, 76 male, mean age 38.3 ± 13.8 years, range 15-77 years) with
dyspeptic symptoms for more than 3 months were studied. All patients' dyspeptic symptoms were recorded before endoscopy. Heartburn and acid regurgitation were not
recognized as dyspeptic symptoms (4). Exclusion criteria were alcohol consumption, use of nonsteroid antiinflammatory drugs, prior gastric surgery, previous H. pylori eradication treatment, upper gastrointestinal malignancy, oesophagitis, peptic ulcer, endoscopic duodenitis and abnormality at biochemical analyses or upper abdominal ultrasonography. Patients were classified according to
predominant symptom as follows; those with epigastric pain (ulcer like dyspepsia), those with symptoms of early satiety - nausea or postprandial fullness (dysmotility like
dyspepsia), those that were not fulfilling for above subgroups (unspecified dyspepsia) (1-4). Control group consisted of 17 non-dyspeptic subjects (9 female, 8 male, mean age 42.9 years, range 25-71). They were underwent upper gastrointestinal endoscopy for iron deficiency anemia, weight loss or the fear of cancer, and did not have any organic lesion. During oesophagogastroduodenoscopy, two biopsy specimens were taken from antral mucosa. Biopsy specimens were fixed 10% formalin. Tissue sections were stained with May Grunwald-Giemsa, and examined under an optical microscope. H.
pylori infection was diagnosed with the observation of the curved, spiral-or-S shaped, violet-blue stained organisms. Bacterial density were not taken into account. Statistical analyses were performed using the Kruskal- Wallis test. Statistical significance was set at p <
0.05. RESULTS Distribution of FD patients to subgroups: There were 111 (63.8%) ulcer like FD, 36 (20.7%) dismotility like FD and 27 (15.5%) unspecified FD patients comprising 174 patients in total. Age, sex, smoking and H. pylori positivity of FD subgroups and control group are shown in Table 1. Groups were found to be similar similar according to age, sex and smoking attributes (p>0.05). H. pylori positivity didn't show a significant difference but it is highest in ulcer like group and lowest in dismotility like group (in order; 77.5%, 61.1%). The average age of patients with ulcer like dyspepsia was lower, but not significant (p >0.05). DISCUSSION H. pylori have a
causal role in the development of peptic ulcer. The eradication of this microorganism prevents relapse of peptic ulcer. However, the controversial
explanations on H. pylori and functional dyspepsia are still lasting (8). Providing that H.
pylori infection has a causal role in development of dyspepsia symptoms, H. pylori prevalence in patients with FD is expected to be higher than in
non-dyspeptic subjects, and dyspepsia symptoms must be relieved by eradication therapies. In the present study we found that H. pylori prevalence
was not significantly different between dyspepsia subgroups and non-dyspeptic persons. This was to confirm Pereira-Lima group results that the frequencies of H. pylori infection
were similar in ulcer like, dismotility like, unspecified dyspepsia groups and controls (9). In Wilhelmsen study H.
pylori infection was diagnosed in 34% patients with FD and 36% controls; the patients had higher psychological scores than normal control regardless of H. pylori status
(10). An investigation carried out on a large Japanese population revealed that there was no significant relationship between H.
pylori infection and any type of FD; symptoms frequency had a tendency to decline with age, while the rate of H.
pylori infection increased with age (11). ERADYS Study Group did not demonstrate any substantial benefit of eradicating H.
pylori in patients with FD. Eradication therapies can cause an improvement in antral gastritis, but the emptying of solids and gastric acid
secretion were not modified (12,13). The study of McColl and colleagues showed that dyspepsia had resolved in 21% of patients treated with omeprazole and antibiotic, 7% of the group were given omeprazole alone one year after the completion of treatment (14). The cure of H.
pylori was seen to be effective in reducing dyspepsia symptoms in employees with H. pylori infection and functional dyspepsia in a Japanese industrial corporation (15). High H.
pylori IgG titers is stated as a risk factor for the subgroup of FD, which is described as frequent dyspepsia (> 6 episode/ recent one year) (16). A multicentric study demonstrated that eradication led to improvement of dyspeptic symptoms in approximately 9% of patients (17) It is possible that the contradictory results related to FD and H.
pylori may be arisen from the differences of
the study groups. The disease overlaps with its own subgroups and other functional diseases of alimentary tract (3,18,19). Therefore, it is difficult to homogenize the research groups and to find a parallelism among groups of different studies. Also the removal of gastroesophageal reflux symptoms and eructation from the dyspepsia description reduced the group similarities among studies. The dyspepsia symptoms of some patients with functional dyspepsia may be related to H. pylori infection,
but our data didn't show any relationship between the major subgroups of functional dyspepsia and H.pylori infection.
|
||
|
|
REFERENCES: 1.
Fisher
RS, Parkman HP. Management of nonulcer dyspepsia. N Engl J Med 1998;
339:1376-81. 2.
Rabeneck
L, Wray NP, Graham DY. Managing dyspepsia: what do we know and what do
we need to know? Am J Gastroenterol 1998; 93:
920-4. 3.
Stanghellini
V, Tosetti C, Paternico A, De Giorgio R, Barbara G, Salvioli B,
Corinaldesi R. Predominant symptoms identify different
subgrouops in functional dyspepsia. Am J Gastroenterol 1999; 94: 2080-5. 4.
Malferteiner
P. Current concepts in dyspepsia: a world perspective. Eur J Gastroenterol
1999; 11(Suppl 1): 25-9. 5.
Tack
J, Piessevaux H, Coulie B, Caenepeel P, Janssens J. Role of impaired gastric accommodation to a meal in functional dyspepsia. Gastroenterology 1998; 115: 1346-52. 6.
Basak
M, Demirtürk L, Yazgan Y, Gürbüz K, Özdogan Y, Kizilkaya E,
Öztürk R, Çankir Z. Nonülser dispepsili hastalarda
Helikobakter pilorinin mide motilitesine etkisi. T
Klin Gastroenterohepatoloji 1998; 9: 7-11. 7.
Friedman
LS: Helicobacter pylori and nonulcer dyspepsia. N Engl J Med 1998;
339:1928-30. 8.
Axon
ATR. Treatment of Helicobacter pylori: an overview. Aliment Pharmacol Ther 2000;
14 (Suppl. 3): 1-6. |
9.
Pereira-Lima
JG, Scholl J, Pinheiro JB, Pereira- Lima L, Reimann JF. Helicobacter pylori-associated gastritis: does it play a role in
functional dyspepsia? Z Gastroenterol 1995; 33: 421-5. 10.
Wilhelmsen
I, Tangen Haug T, Sipponen P, Berstad A. Helicobacter pylori in functional dyspepsia and normal controls. Scand J
Gastroenterol 1994; 29: 522-7. 11.
Kawamura
A, Adachi K, Takashima T, Murao M, Katsube T, Yuki M, Watanabe
M, Kinoshita Y. Prevalence of functional dyspepsia and
its relationship with Helicobacter pylori infection in a Japanese population. J Gastroenterol
Hepatol 2001; 16: 384-8. 12.
Froehlich
F, Gonvers JJ, Wietlishbach V, Burnard B, Hildebrand P, Schneider C,
Saraga E Beglinger C, Vader JP; Eradication in Dyspepsia (ERADYS) Study Group. Helicobacter
pylori eradication treatment does not benefit
patients with nonulcer dyspepsia. Am J
Gastroenterol 2001; 96: 2329-36. 13.
Parente
F, Imbesi V, Maconi G, Cucino C, Manzionna G, Vago L, Bianchi
Porro G. Effects of Helicobacter pylori eradication on
gastric function indices in functional dyspepsia. Scand
J Gastroenterol 1998; 33: 461-7. 14.
McColl
K, Murray L, E-Omar E, Dickson A, El- Nujumi A, Wirz A, et al. Symptomatic benefit from eradicating Helicobacter pylori
infection in |
patients with nonulcer dyspepsia. N
Engl J Med 1998; 339: 1869-74. 15.
Azuma
T, Ito Y, Suto H, Ohtani M, Dojo M, Muramatsu A, Kuriyama M, Kato
T. The effect of Helicobacter pylori eradication therapy
on dyspepsia symptoms in industrial workers in
Japan. Aliment Pharmacol Ther 2001; 15:
805-11. 16.
Holtmann
G, Gschossmann J, Holtmann M, Talley NJ. H. pylori and functional dyspepsia: increased serum antibodies as an
independent risk factor? Dig Dis Sci 2001; 46: 1550-7. 17.
Malfertheiner
P. Helicobacter pylori eradication in functional dyspepsia: new evidence
for symptomatic benefit. Eur J Gastroenterol Hepatol 2001; 13(Suppl2): 9-11. 18.
Talley
NJ, Zinsmeister AR, Schleck CD, Melton LJ. Dyspepsia and dyspepsia subgroups: a population- based study. Gastroenterology 1992;
102: 1259-68. 19.
Agreus
L, Svardsudd K, Nyren O, Tibblin G. Irritable bowel syndrome and dyspepsia
in general population: overlap and lack of
stability over time. Gastroenterology 1996; 110:
969-70. |