Alimentary tract and pancreas
Alimentarni trakt i pankreas
ARCH GASTROENTEROHEPATOL 2002; 21
( No 3 – 4 ):
The relationship between the
density of Helicobacter pylori colonisation and the degree of gastritis
severity
Odnos izmedju denziteta
kolonizacije Helicobacter pylori i
stepena težine gastritisa
1Saša Grgov, 2Milosav Stefanović, 3Vuka Katić.
1Department of Medicine - Unit of Gastroenterology, Health Center Leskovac, 2Department of Pathology, Health Center Leskovac, 3Institute of Pathology, Clinical Center Niš.
Abrevations used in this article:
H. pylori, Helicobacter
pylori; IM, intestinal metaplasia.
Address correspondence to:
Prim. dr sci. med. Saša Grgov
Department of Medicine - Unit of Gastroenterology,
Health Center Leskovac,
116 Svetozara Markovića Str.
YU-16000 Leskovac, Serbia,
FAX + 381 16 247810
Email: [email protected].
....................... ..............................................
H.pylori colonisation and degre of gastritis Gastroenterološka sekcija SLD-
01738, 2002.
ABSTRACT
Upper gastrointestinal endoscopy was performed in 289 H. pylori positive patients. The rapid urease test and histologic examination were used for detection and semiquantitative assessment of H. pylori on endoscopic biopsies of the gastric mucosa. Classical hematoxylin-eosin method and histochemical staining methods (AB-PAS and HID-AB) were used for histologic assessment of gastritis. The results of the study showed that along with the increase of density of H. pylori colonisation there was a tendency of increasing the gastritis activity score in the gastric antrum (p < 0.01) and in the gastric corpus (p < 0.01). A statistically significant decrease of the score of antral atrophy and intestinal metaplasia was determined with the increase of density of H. pylori colonisation in the gastric antrum (p < 0.01 for atrophy; p < 0.05 for intestinal metaplasia). The average value of atrophy score in the corpus did not statistically differ much according to the degree of density of H. pylori colonisation in the gastric corpus. It can be concluded that H. pylori plays the most important part in the occurence and maintenance of the chronic active inflammation in gastric mucosa. Differently from atrophy of the gastric corpus, atrophic and mataplastic milieu in the gastric antrum is an inadequate environment for the survival of H. pylori.
Key words: Helicobacter pylori, gastritis activity, atrophy, intestinal metaplasia.
SAŽETAK
Gornja
gastrointestinalna endoskopija je primenjena kod 289 H.
pylori pozitivnih pacijenata. Za otkrivanje i semikvantitativnu procenu H. pylori na endoskoposkim biopsijama
sluzokože želuca korišćen je brzi ureaza test i histološki pregled. Za
histološku procenu gastritisa korišćena je klasična hematoxylin-eozin metoda i
histohemijske metode bojenja (AB-PAS i HID-AB). Rezultati istraživanja su
pokazali da je sa povećanjem denziteta H.
pylori kolonizacije postojala tendencija povećanja skora aktivnosti
gastritisa u antrumu (p < 0.01) i korpusu želuca (p < 0.01). Utvrđeno je
statistički značajno smanjenje skora atrofije i intestinalne metaplazije u
antrumu sa povećanjem denziteta H. pylori
kolonizacije u antrumu želuca (p < 0.01, za atrofiju; p < 0.05, za
intestinalnu metaplaziju). Srednja vrednost skora atrofije u korpusu nije se
statistički značajno razlikovala po stepenima denziteta H. pylori kolonizacije u korpusu želuca. Može se zaključiti da H.
pylori igra glavnu ulogu u nastanku i održavanju hronične aktivne
inflamacije u sluzokoži želuca. Atrofični i metaplastični milje u antrumu
želuca je nepogodna sredina za opstanak H.
pylori, za razliku od atrofije u korpusu želuca.
Ključne reči: Helicobacter pylori, aktivnost gastritisa, atrofija, intestinalna metaplazija.
By the time H. pylori was identified as the main causative factor of the chronic non-autoimune gastritis numerous classifications of gastritis had been used. The Sydney Classification from 1990 contributed the more simplified approach (1). This classification combined topographic, morphological and aetiologic information in order to establish a clinically useful diagnosis. At the symposium on gastritis held in Houston in 1994, the part of The Sydney Classification related to histologic criteria was corrected, and the addition of the prefix related to aetiology was suggested whenever it was possible (2). According to the Sydney system there are three types of gastritis: acute, chronic and the group of special forms. According to their position they are referred to as antral, corpus gastritis and pangastritis (3).
With chronic superficial gastritis, inflammation is limited to the superficial part of the gastric mucosa. In the course of time, the inflammatory cell infiltrate penetrates deeper between the gastric glands, thus producing a chronic deep gastritis. Both forms of gastritis (chronic superficial and chronic deep) belong to the chronic non-atrophic gastritis (4). With chronic non-atrophic H. pylori gastritis the antrum is always inflamed. The extension of inflammation to the mucosa of the corpus produces pangastritis, which is dominantly antral. After several years or decades, an average third of the patients with chronic non-atrophic gastritis develop chronic atrophic gastritis (5, 6).
Although the genesis of intestinal metaplasia (IM) is vague, it is considered that H. pylori, especially cagA positive species, play an important part in its development. It is possible that the activation of CDX1 and/or CDX2 transcription factors leads to the change in differentiation of gastric epithelial stem cells as well as to the development of an epithelium with intestinal phenotype characteristics (7).
The aim of this prospective study is to examine the relationship between the density of H. pylori colonisation in gastric mucosa and the degree of severity (extent) of certain histologic parameters of gastritis, such as inflammation activity, atrophy and IM.
MATERIAL AND METHODS
PATIENTS This prospective study involved 289 H. pylori positive patients (161, 55.7% male; 128,44.3% female; average age: 47.80 ± 14.39), from whom 136 had duodenal ulcer, 54 had gastric ulcer and 99 had non-ulcer dyspepsia.
The exclusion criteria from the study were as follows: a) therapy with proton pump inhibitors and antibiotics during the past four weeks; b) prolonged nonsteroidal anti-inflammatory drugs medication; c) previous H. pylori eradication therapy; d) previous stomach surgery, with the exception of simple sutures because of ulcer perforation; e) severe associated diseases; f) excessive long-lasting alcohol abuse; g) pregnancy and lactation; h) complications of gastric and duodenal ulcer disease (active ulcer bleeding and peptic stenosis of the duodenum).
The following methods of research were used: upper gastrointestinal endoscopy, H. pylori biopsy urease test, histologic examination of endoscopic gastric mucosal biopsies and statistical analysis.
Endoscopy
and biopsy After
six-hour fast, proper purgation and disinfection of the instrument, with the
previous local pharyngeal anesthesia with 10% Xylocain, upper gastrointestinal
endoscopy with mucosal biopsies, taken with a standard forceps, were performed.
Eight gastric mucosal biopsies were taken: two of them for rapid H. pylori urease test (an antral, 20 mm
away from the pylorus toward the great curve, and a fundic) and 6 biopsies for
histologic examination (three from the antrum, at least 20 mm from the pylorus,
from the anterior and posterior walls and from the incisura angularis, and 3
biopsies from gastric corpus/fundus - the anterior and posterior wall). In
patients with gastric ulcer, four additional biopsies were taken from the edges
and basis of ulcer in order to exclude malignity.
To avoid or reduce the possibility of cross-contamination, the biopsy forceps were washed up with water whenever biopsy forceps passed from one segment of mucosa to another.
For detection of H. pylori on endoscopic biopsies, rapid urease test (Bramio H. pylori test, The Institute for Immunology and Virology - Torlak, Belgrade) and histologic examination were used. H. pylori status was regarded positive if both tests were positive. The result of the urease test was read after 1, 3 and 24 hours. The test was regarded positive if the colour changed from yellow to red. For identification and semiquantitative evaluation of H. pylori status by histologic examination, endoscopic mucosal biopsy samples were fixed in the standard 10% formalin for 24 hours. After that, the tissue was routinely processed, embedded in paraffin and cut by microtom up to the thickness of 4mm. After the deparaffinisation and processing in grade alcohol, selected clippings were stained by hematoxylin-eosin (HE) and Giemsa. H. pylori colonisation density was determined semiquantitatively in the interval from 0-3 (0, absence of H. pylori; 1, small number of H. pylori focally; 2, large number of H. pylori focally or small number, diffusely; 3, large number of H. pylori diffusely) (8). During the histologic evaluation, the pathologist was not informed about the urease test.
For histologic evaluation of gastric musosa, the classical HE staining method was used. In cases of the presence of IM in the stomach, specific histochemical staining methods were used to show the type and amount of epithelium mucines: AB-PAS (alcian blue-periodic acid Schiff) for verification of weakly acid sialomucines and neutral fucomucines; HID-AB (high iron diamine-alcian blue), pH-2.5 for verification of highly acid sulphomucines and weakly acid sialomucines. The following histologic changes of the mucosa of gastric antrum and corpus were analysed: activity of inflammation, atrophy and IM. The changes were graded according to modified Sydney system from 0-3 : 0, absence; 1, easy; 2, medium; 3, severe (9).
Statistical analysis The results are
graphically shown according to the methodology of descriptive statistic. In
order to verify the hypotheses and determine the significance of the
differences between certain parameters, specific statistic tests were applied,
such as Mantel-Haenszel’s c2
test with Yates’s correction and Fisher’s test of exact probability of zero
hypothesis. With parallel analysis of three or more groups of independent data the
analysis of variance was applied with Post-hoc analysis by
Student-Newman-Kuels’s test. The differences between certain parameters were
considered significant for values p < 0.01 and p < 0.05, and not
significant for values p > 0.05. We also calculated the relative ratios and
risk indices, such as cross-ratio or odds ratio (OR) and relative risk (RR),
with the confidence interval of 95% (95% CI).
RESULTS
From 289 H. pylori positive patients, 216 (74.7%) had H. pylori only in the antrum, and 30 (10.4%) only in the gastric corpus, p < 0.01 (OR=25.55, 95%CI: 15.73-41.71; RR=7.20, 95%CI: 5.10-10.17). In 43 of 289 (14.9%) patients H. pylori was detected both in the antrum and gastric corpus. In the gastric antrum, 108 patients had the density of H. pylori colonisation 1+, 116 were with the density 2+ and 35 had the density 3+. In the gastric corpus, 62 patients were with the density 1+ and 11 with the density 2+.
Using the analysis of variance with Post-hoc analysis by Student-Newman-Kuels’s test statistically significant difference was determined among the average score values of gastritis activity in the gastric antrum according to the density of H. pylori colonisation in the antrum (F=30.60, p< 0.01), which is the result of the statistically significant difference in all the comparisons, with the exception of the score difference between the zero (2.00 ± 0.66) and the first degree (1.90 ± 0.66) density of colonisation. Figure 1.
Also, a statistically significant difference in average score values of gastritis activity was determined in the gastric corpus according to the levels of density of H. pylori colonisation in the corpus (F=20.27, p < 0.01). Such a result is a consequence of statistically significantly higher score of activity at the first (1.76 ± 0.52) and the second degree (2.14 ± 0.69) of colonisation density, in relation to the zero degree (1.15 ± 0.36), while the score difference between the first and the second degree of density was not statistically important. Figure 2.
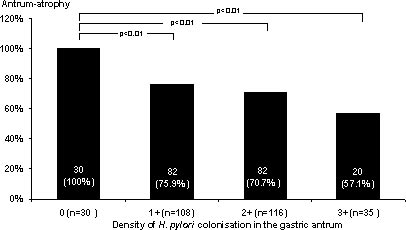
The greatest frequency of atrophy in the gastric antrum was at the zero degree of density of H. pylori colonisation in the antrum (n=30 or 100%) and it statistically differed much in relation to the frequency of atrophy at the first degree of density (75.9%, p < 0.01; RR=1.32, 1.18-1.46), the second degree (70.7%, p < 0.01; RR=1.41, 1.26-1.59) and the third degree of density (57.1%, p < 0.01; RR=1.75, 1.31-2.33). The difference in frequency of atrophy between the first, second and the third degree of colonisation density was not statistically significant. Figure 3A.
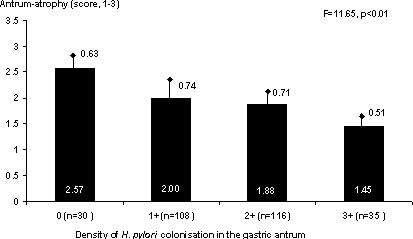
A statistically significant difference was determined between the average score values of atrophy in the gastric antrum according to the degrees of density of H. pylori colonisation in the antrum (F=11.65, p < 0.01) - all the differences in the score of atrophy were statistically significant according to the degrees of colonisation density, with the exception of the difference between the first and second degree of density. The average score value of atrophy in the antrum decreased with the rise of the degree of density of H. pylori colonisation. Figure 3B.
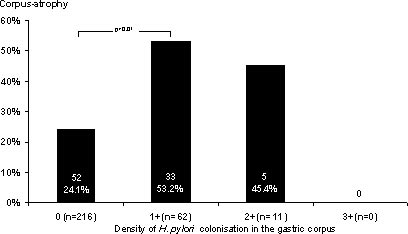
There was a statistically significant difference in the frequency of atrophy in the gastric corpus between the zero (24.1%) and the first degree of density of H. pylori colonisation (53.2%), p < 0.01 (OR=0.28, 0.15-0.52; RR=0.45, 0.32-0.63), while the difference in the frequency of atrophy between the zero and second, as well as between the first and second degree of colonisation density was not statistically significant. Figure 4A.
The average score value of atrophy in the corpus did not statistically differ much according to the degrees of density of H. pylori colonisation in the gastric corpus (F=1.70, p > 0.05). Figure 4B.
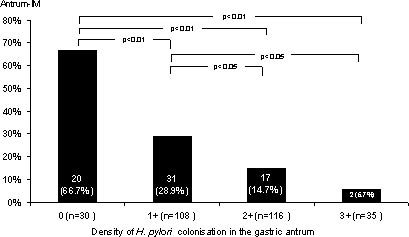
Frequency of antral IM was greatest at the zero degree of density of H. pylori colonisation in the antrum (66.7%) and it statistically differed much in relation to the frequency of IM at the first degree of density (28.9%, p < 0.01; OR=4.97, 1.94-12.97; RR=2.32, 1.57-3.43), the second degree (14.7%, p < 0.01; OR=11.65, 4.27-32.55; RR=4.55, 2.74-7.55) and at the third degree of density (5.7%, p < 0.01; OR=33.0, 5.78-248.06; RR=11.67, 2.97-45.88). Also, the frequency of IM statistically differed much between the first and the second degree of density (p < 0.05; OR=2.34, 1.15-4.80; RR=1.96, 1.15-3.33), as well as between the first and the third degree of density (p < 0.05; OR=6.64, 1.42-42.65; RR=5.02, 1.27-19.93) while the difference in frequency of IM between the second and third degree of density of H. pylori colonisation was not statistically significant. Figure 5A.
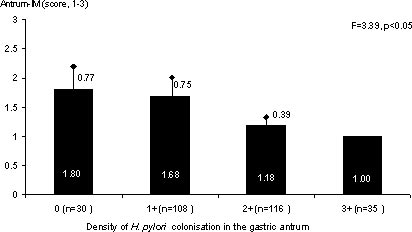
A statistically significant difference was determined between the average score values of IM according to the degrees of density of H. pylori colonisation in the gastric antrum (F=3.39, p < 0.05), which is the result of the statistically significant difference between the score at the zero and the second, as well as the first and the second degree of density, while all other differences did not statistically differ much. Figure 5B.
DISCUSSION
Analysing certain histologic parameters of gastritis according to the rates of density of H. pylori colonisation, we have noticed that the score of gastritis activity in the gastric antrum had a tendency of increasing with the higher rate of antral density of H. pylori colonisation. The average value of the gastritis activity score in the corpus also increased with the increase of the H. pylori colonisation density rate in the corpus.
A study which included 107 patients suffering from dyspepsia, from Finland, pointed to the existence of a positive correlation between the density of H. pylori colonisation and the rate of inflammation and gastritis activity in the gastric antrum, while in the gastric corpus there was only a positive correlation between the gastritis activity and the density of H. pylori colonisation (10).
According to the study carried out by Satoh et al. which included 314 patients, a positive correlation was found between the density of H. pylori colonisation and the rate of polimorphonuclear infiltration in lamina propria as well as in the superficial epithelium of gastric antrum and corpus (11). There was a lower degree of correlation between the density of H. pylori colonisation and the mononuclear cell infiltration.
Other authors also point out that the degree of mononuclear and polimorphonuclear infiltration, the degree of degeneration and regeneration of the superficial epithelium, and the degree of mucine depletion are in correlation with the density of H. pylori colonisation (12).
In 1000 biopsy samples taken from 10 topographic locations in the stomach, from 50 patients, Bayerdörffer at al. showed that the area of H. pylori colonisation was greater than the area of polimorphonuclear infiltration, which suggests that H. pylori colonisation precedes the development of active gastritis (13).
On the basis of our study as well as the studies of other authors, we can conclude that H. pylori plays the main part in the occurrence and maintenance of the chronic active inflammation in the mucosa of gastric antrum and corpus.
The eradication of H. pylori infection leads to the resolution of inflammation and gastritis activity. Inflammation of low degree can persist 6-18 months after the eradication of the infection (14-17).
Polimorphonuclear infiltration (gastritis activity) can be an important factor of the occurrence of later consequences of H. pylori infection, such as atrophy. This is based on the fact that neutrophils are capable causing the damages of the gastric gland and the superficial epithelium by mediating the reactions of the free toxic radicals or by influencing the releasing of reactive oxygen metabolites from the inflammatory cells. The damages of DNA caused by oxygen radicals lead to the modification of genes with a potential mutagenic and carcinogenic effect. For human cancer, including gastric adenocarcinoma, the most important changes are those of ras-family of proto-oncogene and p53 tumour suppressor gene (18). Sensitive marker of oxidative damage of DNA cells of the affected organ represents 8-hydroxideoxiguanosin, which originates from deoxiguanosin under the influence of the free oxygen radicals (19).
Several years long presence of H. pylori can lead to irreversible mucosal damage which lead to the loss of epithelium and mucosal glands (20). The destroyed gastric glands can be replaced by deposition of extracellular matrix, fibroblast and, eventually collagen - this variant of atrophy is marked as fibrosis. During the synchronous and metachronous reparation processes the destroyed gastric glands may be exchanged with the intestinal type of epithelium and glands (IM) or with glands which are normally located in other part of the stomach (pseudopyloric metaplasia of the corpus mucosa) (21).
Neutrophil infiltration is especially pronounced in the so called neck zone of mocosal glands, a special zone of cell replication which participates in regeneration of the cover epithelium and the gastric glands. Apart from the strict positive correlation between H. pylori density and chronic inflammatory cell infiltrate, Lynch et al. found a close positive correlation between H. pylori colonisation density and epithelial proliferation, concluding that H. pylori increases the gastric epithelial proliferation through mucosal inflammatory response, though there may be other mechanisms, which may play a part in the gastric carcinogenesis (22).
In our patients, the frequency of the gastric antrum mucosal atrophy decreased with the increase of the H. pylori colonisation rate. Also, there was a tendency of decreasing the average value of the atrophy score with the increase of the rate of H. pylori colonisation density in the antrum (p < 0.01). Frequency of IM in the gastric antrum had a statistically significant drop with the increase of the rate of H. pylori colonisation density in the antrum. Also, the score of IM showed the tendency of decreasing with the increase of the rate of H. pylori colonisation density in the gastric antrum (p < 0.05).
Our studies match the data in literature on the fact that the prolonged atrophy causes a spontaneous loss of H. pylori from the gastric mucosa and the later drop of the H. pylori antibodies titer. As the atrophy and IM become more severe and more extensive, the density of H. pylori colonisation is reduced because of the occurrence of hypoacidity and predominance of other microbes (23). These microbes turn food nitrates into nitrites thus leading to formation of N-nitroso compounds, i.e., N-nitrosoamins, primary carcinogens of stomach cancer (18).
In our patients,
the average atrophy score value in the corpus did not statistically differ much
according to the rate of H. pylori colonisation
density in the gastric corpus, that is, there was no tendency of decreasing the
average value of the atrophy score with the increase of H. pylori colonisation density like in the gastric antrum. Normal
acidity disables bacteria in the corpus to survive. Presence of the corpus
atrophy leads to the reduction of the mass of parietal cells and to the
occurrence of acid hiposecretion. According to scarce data in literature, such
atrophic milieu in the corpus is, unlike the atrophic milieu in the antrum, a
suitable environment for H. pylori
colonisation (24). However, the question is what the distribution of H. pylori colonisation and its density
are like in the gastric corpus under the conditions of significant expansion of
antral type of mucosa toward the corpus (pseudopyloric metaplasia). In order to
answer this question, wide endoscopic and histologic prospective studies are
needed.
REFERENCES:
1.
Misiewicz JJ, Tytgat GNJ, Goodwin CS, et al. The
Sydney system: a new classification of gastritis. Word Congress on
Gastroenterology. Working Party Reports. Sydney, Blackwell Sci Publ, 1990;
1-10.
2.
Sipponen
P, Kekki M, Seppälä K, Siurala M. The relationships between
chronic gastritis and gastric acid secretion. Aliment Pharmacol Ther 1996; 10
(Suppl 1): 103-18.
3.
Price
AB. The
Sydney system: histologic division. J Gastroenterol Hepatol 1991; 6: 209-22.
4.
Gonzaga Vaz Coelho L,
León-Barúa R, and Quigley EMM. Latin-American consensus conference on Helicobacter pylori infection. Am J
Gastroenterol 2000; 95: 2688-91.
5.
Stolte
M, Stadelmann O, Bethke B, Burkard G. Relationship between the degree of Helicobacter pylori colonisation and the
degree and activity of gastritis, surface epithelial degeneration and mucus
secretion. J Gastroenterol 1995; 33: 89-93.
6.
Villako
K, Kekki M, Maaroos H-I, Sipponen P, Uibo R. Chronic gastritis: progression
of inflammation and atrophy in a six-year endoscopic follow-up of a random
sample of 142 Estonian urban subjects. Scand J Gastroenterol 1991; 26 (Suppl
186): 135-41.
7.
Solcia
E, Luinetti O, Villani L, Quilici P, Klersy C and Fiocca R.
Intestinal metaplasia: types, mechanisms of origin, and role in gastric
cancer histogenesis. In: Hunt RH and
Tytgat GNJ. Helicobacter pylori –
basic mechanisms to clinical cure 2000. Dordrecht. Kluwer Academic 2000: 249-54.
8.
Talamini G, Zamboni G, Cavallini G. Antral mucosal Helicobacter pylori infection density as
a risk factor of duodenal ulcer. Digestion 1997; 58: 211-7.
9.
Dixon MF, Genta RM, Yardley
JH, Correa P.
Participants in the international workshop on the histopathology of gastritis.
Classification and grading of gastritis: the updated Sydney system. Am J Surg
Pathol 1996; 20: 1161-81.
10.
Karttunen
T, Niemelä S, Lehtola J. Helicobacter pylori in dyspeptic patients:
quantitative association with severity of gastritis, intragastric pH, and
serum gastrin concentration. Scand J Gastroenterol 1991; 26 (Suppl 186):
124-34.
11.
Satoh
K, Kimura K, Yoshida Y, Kasano T, Kihira K, and Taniguchi Y. A
topographical relationship between Helicobacter
pylori and gastritis: quantitative assessment of Helicobacter pylori in th gastric mucosa. Am J Gastroenterol 1991;
86: 285-91.
12.
Sipponen
P, Stolte M. Clinical impact of routine biopsies of the gastric
antrum and body. Endoscopy 1997; 29: 671-8.
13.
Bayerdörffer
E, Oertel H, Lehn N, et al. Topographic association
between active gastritis and Campylobacter pylori colonization. J Clin Pathol
1989; 42: 834-9.
14.
El-Omar EM, Oien K, Murray LS, et al. Increased prevalence of precancerous changes
in relatives of gastric cancer patients: critical role of H. pylori. Gastroenterology 2000; 118: 22-30.
15.
El-Omar
EM, Oien K, El-Nujumi A, et al. Helicobacter pylori
infection and chronic gastric acid hyposecretion. Gastroenterology 1997; 113:
15-24.
16.
Van der Hulst RWM, van der Ende
A, Dekker FW, et al. Effect of Helicobacter pylori
eradication on gastritis in relation to cagA: a prospective 1-year follow-up
study. Gastroenterology 1997; 113: 25-30.
17.
De Francesco V, Zullo A,
Rinaldi V, et al. Relationship between antral lymphocyte density and basal gastrin
levels in patients with Helicobacter
pylori infection. Digest Liver Dis 2000; 32: 676-81.
18.
Zhang ZW and Farthing MJG. Helicobacter pylori in gastric malignancy: role of oxidants, antioxidants
and other co-factors. In: Hunt RH
and Tytgat GNJ. Helicobacter pylori
– basic mechanisms to clinical cure 2000. Dordrecht. Kluwer Academic 2000:
513-24.
19.
Hahm
KB, Lee KJ, Kim JH, Cho SW, and Chung MH. Helicobacter
pylori infection, oxidative DNA damage, gastric carcinogenesis, and reversibility
by rebamipide. Dig Dis Sci 1998; 43: 72-7.
20.
Fiocca
R, Luinetti O, Villani L, Chiaravalli AM, Capella C, Solcia E.
Epithelial cytotoxicity, immune responses, and inflammatory components of Helicobacter pylori gastritis. Scand J
Gastroenterol 1994; 205: 11-21.
21.
Genta
RM. Can atrophic gastritis be diagnosed in the presence of
Helicobacter pylori infection? In: Hunt RH and Tytgat GNJ. Helicobacter pylori – basic mechanisms
to clinical cure 2000. Dordrecht. Kluwer Academic 2000: 229-37.
22.
Lynch DA,
Mapstone NP, Clarke AM, et al. Correlation between
epithelial cell proliferation and histological grading in gastric mucosa. J
Clin Pathol 1999; 52: 367-71.
23.
Komoto
K, Haruma K, Kamada T, et al. Helicobacter pylori infection and gastric neoplasia: correlations
with histological gastritis and tumor histology. Am J Gastroenterol 1998; 93:
1271-6.
24.
Larkin
CJ, Watson RGP, Sloan JM, Stevenson M, Ardill JES and Buchanan D.
Distribution of atrophy in Helicobacter
pylori-infected subjects taking proton pump inhibitors. Scand J
Gastroenterol 2000; 35: 578-82.
GRGOV
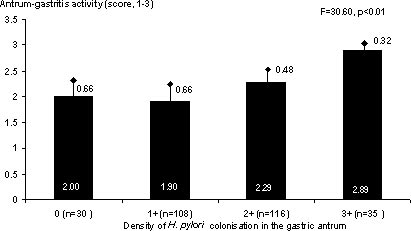
Figure
1. The average value of gastritis activity score in the antrum in relation to
the rate of H. pylori colonisation
density in the gastric antrum.
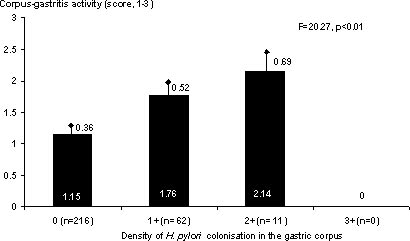
Figure
2. The average value of gastritis activity score in the corpus in relation to
the rate of H. pylori colonisation
density in the gastric corpus.
![]()
![]()
Figure
3. (A) The frequency of atrophy and (B) the average value of
atrophy score in the antrum in relation to the rate of H. pylori colonisation density in the gastric antrum.
![]()
![]()
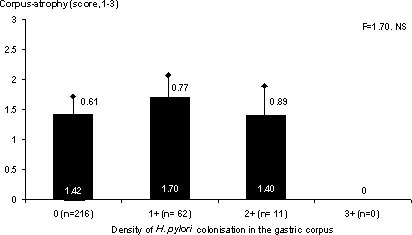
Figure
4. (A) The frequency of atrophy and (B) the average value of
atrophy score in the corpus in relation to the rate of H. pylori colonisation density in the gastric corpus.
![]()
![]()
Figure
5. (A) The frequency of intestinal metaplasia (IM) and (B) the average value of
IM score in the antrum in relation to the rate of H. pylori colonisation density in the gastric antrum.