Liver and biliary tract
Jetra
i bilijarni trakt
ARCH GASTROENTEROPHEPATOL 2002; 21 ( No 3 – 4 ):
Coagulation disorders in decompensated liver cirrhosis and
their prognostic value
Koagulacioni poremećaji u dekompenzovanoj cirozi jetre i njihov prognostički značaj
( accepted December 15th, 2002 )
1Gradimir
Golubović, 1Ratko Tomašević, 1Lidija Burg, 2Slavica
Spasić,
3Tamara Aleksić, 3Nikola Milinić
1
Department of Gatroenterology, Clinical Hospital Center Zemun, Belgrade,
2
Institute of Biochemistry, Medical Faculty, University of Belgrade,
3
Department of Gastroenterology, Clinical Hospital Center Bezanijska Kosa,
Belgrade.
Address
correspondance to:
Professor
Dr Gradimir Golubović
Department
of Gastroenterology
Clinical
Hospital Center Zemun
9
Vukova Str.
YU-11080
Belgrade, Serbia,
Yugoslavia
............................ ........................................................
Cagulation
disorders in cirrhosis
Gastroenterološka sekcija SLD-
01739,
2002.
Abstract
Disorders
of haemostasis are frequent in the diseases of the liver, and are in
correlation with the degree of liver insufficiency. As a result, bleeding
occurs, which, at long end, affects prognosis and life duration in these
patients. The aim of this study is to
evaluate mean values of some factors of coagulation (factor II, V, VII) and
coagulation inhibitors (Anti-thrombin III,AT-III) in 69 patients with
decompensated alcoholic liver cirrhosis (Child C) and to determine the
influence of coagulation disorders on the onset of bleeding and survival
rate.
We
came to conclusion that there was no significant difference in level of
coagulation factors and inhibitors between
bleeding and non-bleeding patients, although the mean values of
investigated parameters were 50% lower
for coagulation factors and 60% for coagulation inhibitors in bleeders. The
reason for this result we found in positive correlation in decreasing both factors
and inhibitors, which agrees with hypothesis that in these cases haemostasis is
regulated on new, lower level. Patients with final lethal outcome had
significantly low level of AT-III was we considered as an important predictive
factor in our series. This results show complex interrelation between
haemostasis factors, bleeding, quality of life and survival rate in patients
with decompensated liver cirrhosis
Kez
words: coagulation
factors, ainti-trombin III, cirrhosis.
Sažetak
U hroničnim bolestima jetre poremećaji
hemostaze su u korelaciji sa stepenom insuficijencije jetre. Kao rezultat toga,
u krajnjoj konsekvenci krvarenje bitno utiče na finalni ishod odnosno duzinu
prezivljavanja osoba sa hroničnim bolestima jetre. Cilj ove studije je da se ispitaju prosečne
vrednosti činioca koagulacije ( faktori II,V,VII ) i inhibitora koagulacije (
Anti-trombin III ) u 69
bolesnika sa dekompenzovanom alkoholnom bolešću jetre te da se odredi uticaj
deficitnog procesa koagulacije na pocetak krvarenja i prezivljavanje ovih
bolesnika.
Zaključak ove studije je da ne postoji
značajna razlika u nivoima faktora koagulacije i inhibitora koagulacije izmedju
pacijenata koji su krvarili i onih koji nisu krvarili, premda je prosečna
vrednost faktora koagulacije bila niza 50% a inhibitora koagulacije 60% od
prosečnih vrednosti. Objašnjene ovoga rezultata je da je prosečno sniženje
faktora i inhibitora koagulacije bilo proporcionalno te da je potvrdjena
hipoteza da u bolesnika sa cirozom jetre hemostaza je regulisana na novom, nizem
nivou. Tokom perioda ispitivanja u trajanju od 30 meseci, u osoba sa letalnim
ishodom nizak nivo AT-III je
bio dobar pokazatelj loše prognoze. Rezultati ove studije ukazuju na kompleksnu
interakciju izmedju činioca hemostaze, krvarenja, kvaliteta zivota i
prezivljavanja u pacijenata sa dekompenzovanom cirozom jetre.
Ključne reči: činioci koagulacije,
anti-trombin III,ciroza.
Abnormal clotting in patients with liver cirrhosis is caused by dearranged coagulation pofile what increases the risk of gastrointestinal (GI) bleeding or/and thrombosis (1). Thrombocitopaenia and disordered platelet activity have an important additional role in bleeding diathesis. Disseminated intravascular coagulation (DIC), and accelerated fibrinolysis, together with altered hepatic clearance are more likely to cause bleeding (2). \
Gastrointestinal
bleeding is an important and life-threatening complication of decompensated
liver cirrhosis (3). Mostly it is due to
ruptured oesophageal varices, hypertensive gastropathy and peptic ulcers, while
bleeding in urogenital tract, central
nervous system and skin area is less common (9). There is an evidence
that in liver cirrhosis decreased synthesis of coagulation factors itself is
not enough to initiate bleeding, because hemostasis is regulated and maintained
on new, lower level due to decreases synthesis of both coagulation factors and
coagulation inhibitors (5).
Prognosis
after GI is mostly dependent on residual liver function, degree of portal
hypertension and initial cause of bleeding. The worst prognosis is in cases of
ruptured oesophageal varices, where only 50% of patients survive the first
episode of bleeding.
In
this study we investigated the influence of coagulation factors level (F II, F
V and F VII), and coagulation inhibitor antithrombin III (AT-III) on bleeding
and survival rate in patients with decompensated alcoholic liver cirrhosis and
their relationship.
PATIENTS AND METHODS
From
January 1995 until December 2000, 69 patients (45 males,24 females; mean age 54
years) with decompensated alcoholic liver cirrhosis were studied at the
Department of gastroenterology, Medical Center "Zemun",
Belgrade. The diagnosis was made on the
basis of anamnesis, clinical and laboratory investigations, abdominal ultrasonography, abdominal CT, and
liver biopsy (in 10 cases). All patients, according to Child-Pough
classification, were in stage C: hepatosplenomegaly, ascites, encephalopathy,
oesophageal varices, gradus II (44 patients), and gradus III (25 patients).
Mean value of bilirubin (`x=56±12), ALT (x=76+12), and GGT(x=146+21) was
increased while mean value of serum albumin (x=26+4) was decreased. Mean platelet count was 101 000. In 6 patients
parallel hepatitis B virus infection was diagnosed; 5 patients were hepatitis C
positive by serology. Patients had a history of drinking in average of 16
years, and quantity of ingested alcohol varied from 120 to 160 mg/24h.
Patients were followed for 30
months, and during that period episodes of bleeding were monitored together with cause of bleeding.Table 1.
Table 2 shows survival rate and causes of death during follow up period.
Biochemical parameters were obtained by standard methods using B 18 AVL Company
Analyzer. Coagulation factors (F II, F V, F VII) and inhibitor (AT-III), were
determined by coagulation method on automated coagulometer
ACL
300 (Behring technique). Values of coagulation factors and inhibitors are
presented by percents of normal range values, obtained from control group of
healthy individuals (n=30). The correlation between haemostasis status,
bleeding and survival rate were investigated, and importance of each
coagulation factor and inhibitor and their interrelation was evaluated.
Mean values and standard deviation
presented values of these parameters. Data were statistically processed by
using Student's T- test and variation analysis, with results shown in tables.
Interrelation of investigated parameters was evaluated by using linear
regression analysis, and results are presented graphically.
RESULTS
During
the whole follow-up period of 30
months, 22 (32%) patients experienced
one or more bleeding episodes. In 16 (73%)cases, the cause bleeding was
oesophageal variceal haemorrhage. Twenty nine (42%) patients eventually died. Leading cause of
death was GI bleeding and hepatic coma
(12 patients, 41%), hepatic coma alone in 8 (28%) patients, massive GI bleeding
and cirrculatory insufficiency in 3(10%) patients. Table 2.
In
all patients significant decrease of coagulation factors was found: factor VII
(50%), factor II (51%) and factor V (54%). Deviation from normal range for
AT-III was more significant than for each coagulation factor (40%). Positive
correlation between values of F II, F V, F VII and AT-III was determined or, in other words,
decrease in coagulation factors is accompanied with decrease in level of AT-III
(AT-III vs. FII: r=0,604; AT-III vs. FV: r=0,537 and AT-III vs. F VII:
r=0,526). Figure 1, 2, 3.
We
found no significant difference between clotting parameters and AT-III (n=22)
and bleeding rate among bleeders and non-bleeders (n=47). Table 4. Significant difference in values of AT-III
was found between the group of patients who eventually died and those who
survived, while there was no statistically significant difference in values of
F II, FV, and F VII. Table 5. There were no difference between
coagulation parameters and their relation to bleeding and survival rate. Table
6.
DISCUSSION
Portal
hypertension is the most common cause of GI bleeding in decompensated liver cirrhosis
(4). Traditionally it is considered that the risk of bleeding is the most
frequent in Child C stage and depends on grade of oesophageal varices, hepatic
venous pressure gradient and residual liver functions. Disordered haemostasis
play an important additional role in increasing the risk of GI bleeding and
closely correlates with liver insufficiency
(4,7). Kelly D.A. from Birmingham,s Children Hospital
considers that the risk of bleeding in
liver diseases is individual for
each patient and depends on balance of haemostatic parameters synthesis on one
side, and hepatic clearance on the other (8,9). The role of each of these
parameters itself on the onset of bleeding is not yet clear (10).
Our study did not show clear cut
relationship between level of F II, F V, F VII, AT-III and GI bleeding rate,
although their absolute values were decreased for about 50%, and 60% for AT-III. In patients with liver
insufficiency De Katerina reported lower coagulation inhibitors (AT-III,
protein C, protein S) than F VII and prothrombin time (PT), what we were able
to confirm in our series. According to same author, critical point for
gastrointestinal bleeding is Child B stage of cirrhosis, with low level of
coagulation inhibitors when variceal bleeding occur (13). We dmonstrated during
the follow up period patients with Child C cirrhosis bled less frequently
(32%), and that the most common cause of bleeding was oesophageal variceal
rupture (73% of patients). There is some avidence that in cirrhotics variceal bleeding is in
correlation with hypercoagulability state due to haemostatic disbalance caused
by coagulation inhibitors depression thus leading to DIC and secondary
fibrinolysis (11,12). In our study only one patient had DIC, fibrinolysis and
gastrointestinal bleeding. Rodzynek et al. report that normal values of AT-III
is always a good sign of preserved liver functions, and, as liver disease
progress, it's value decreases further (14). Similar observation was reported
by Vukovich reported decreased AT-III and protein C in relation to hepatic
insufficiency progression (1).
In
decompensated liver cirrhosis decrease of coagulation inhibitors is more
pronounced than coagulation activators.
Since there is negative correlation of level of D-dimmer (higher than
reference values) to AT-III and protein C (lower than reference values) several
authors came to conclusion that enhanced fibrinolysis is a consequence of
decreased clearance of plasminogen activators (high PAP), and not due to low
AT-III and PC.
It
is not yet clear why patients with Child C cirrhosis bleed relatively less
frequently, although they have lower level of coagulation factors. The answer
may be in more pronounced decrease of coagulation inhibitor(s) (AT-III - 60% of
normal range) then of coagulation activators what is lessening the risk of
bleeding. According to our investigation in patients with Child C cirrhosis
AT-III stands in close relationship with lethal outcome, and no correlation was
found with coagulation factors, although their values is low, too. AT-III would than be a predictive factor in
our patients who died. Black et al. found that patients with low AT-III and
high bilirubin did not survive more than 6 months, so they consider AT-III a
prognostic index (22).
It
is reported by Osterud that F VII and its activation is a key moment in process
of coagulation (16). The deficit of activated F VII and onset of bleeding is,
according to this author, the best marker of severity of liver lesions, and is
considered to be a sign of bad prognosis. Violi et al. reported that 93% of
patients with F VII level lower than 34% die within 10 months from start of
follow-up, and considers F VII an important predictive factor of survival in
patient with liver disorder. Low levels of F II and FV, inspite of vitamin K
supplementation are bad prognostic sign according to Ekindjian et al (18).
Levels of F V lower than 50% of normal range, these authors liasied with
bleeding episodes (18).
In
conclusion, there is an evidence that the level of AT-III is bad prognostic
indicator in liver diseases. The newly established balance between coagulation
factors and coagulation inhibitors reflects, more or less appropriate
homeostatic balance between pro- and anti-coagulants in Child C cirrhosis what
influences the propensitty to gastrointestinal bleeding.
REFERENCES
1. Vukovich Th, Teufelsbauer H, Fritzer M et al. Hemostasis in patients with liver cirrhosis. Thromb Res 1995; 77:271-28.
2. Kelly DA and Summerfield JA. Hemoestasis in liver disease. Semin Liver Dis 1987; 7: 182-91.
3. Boks AL, Bromer EJP, Schalm SW et al. Hemostasis and fibrinolysis in severe liver failureand their relation to hemorrhage. Hepatology1986; 6. 79-86.
4. Christensen E, Krintel JJ, Hansen SM, Johansen Jk and Juhl E. Prognosis after first episode gastrointestinal bleeding or coma in cirrhosis. Scand J Gastroenterol 1989; 24: 999-1006.
5. Sherlock Sh. The haematology of the liver disease. In: Sherlock Sh. And Dooley J (eds). Tenth ed. London Blackwell Science 1997; p:43-62.
6. Smith
JL. Graham DY. Variceal haemorrhage. A critical evaluation of survival
analysis. Gastroenterology; 1982;
82: 968-73.
7. Zurborn KH, Gram J, Rohwedder E, Bewing B, Bruhn HD. The effect of liver cirrhosis on activation of the coagulation and fibrinolysis system and on coagulation inhibitoris. Med Klin 1989; 84: 515-8.
8. Kelly
DA and Tuddenham EGD. Haemostatic problems in liver disease. Gut 1986; 27: 339-49.
9. Baklaja R. Acquired blood clotting disorders. In: Baklaja R, Pešić MČ and Czarnecki J. (eds). Haemostasis and haemorrhagic disrders. Bad Harzburg, Thymus Med. Fachbuchverlag 2000; pp 104-28.
10. Mammen EF. Coagulation defects in liver disease. Med Clin North Am 1994; 78: 545-54.
11. Bertaglia E, Belmont P, Vertolli U, Martines D. Bleeding in cirrhotic patients. Haemostasis 1983;13: 328-34.
12. Hiller E, Hegemann F, Possinger K. Hipercoagulability in acute variceal bleeding. Thromb Res 1981; 22: 243-51.
13. De Katerina M TarantinoG, Farina C et al. Haemostasis unbalance in Pugh scored liver cirrhosis: Characteristic changes of plasma levels of protein C versus protein S. Haemostasis 1993; 23: 229-35.
14. Rodzynek
JJ, Urbain D, Leautaud P, Wettendorff P and Delcourt A. Antithrombin III,
plasminogen and alfa-2-antipasmin in jaundice. Clinical usefulness and
prognostic significance. Gut 1984;
25: 1050-6.
15. Sauerbruch T. Weinzierl M, Kopcke W et al. Long term sclerotherapy of bleeding esophageal verices in patients with liver cirrhosis. An evaluation of mortality and rebleeding risk factors. Scand J Gastroenterol 1985; 20: 51-8.
16. Osterud B. Factor VII and haemostasis. Blood Coagul Fibrinolysis. 1990; 1: 175-82.
17. Violi F, Ferro D, Basili S et al. Association between low grade disseminated intravascular coagulation and endotoxemia in patients with liver cirrhosis. Gastroenterology 1995; 109: 531-9.
18. Ekindjian OG, Devanley M, Duchassaing D et al . Multivariante analysis of clinical and biological data in cirrhotic patients. Application of prognosis. Eur J Clin Invest 1981; 11: 213-40.
19. D
Amico G G, Morabito A, Pagliaro L et al. Survival and prognostic indicators in
compensated and decompensated liver cirrhosis. Dig Dis Sci 1986; 31: 486-73.
20. Violi F, Ferro D, Basili S et al. Hyperfibrinolysis increases the risc of gastrointestina hamorrhage in patients with advanced cirrhosis. Hepatology 1992; 15: 672-6.
21. Chedid
A, Medenhall CL, Gartside P et al. Prognosti factors in alcoloholic liver
disease. Am J Gastroenterol 1991;
86: 210-6.
22. Black E, Thomsen AC, Hansen T et al. Antithrombin
III-diagnostic and prognostic value in patients with hwpatobilliary disease. Abstract C 10/10.
23. Aurosseau MH, D Angeli JL, Jossas A. Antithrombin III versus prothrombin in liver cirrhosis. Haemostasis. 1981; 10: 104-7.
24. Papatheodoridis GV, Patch D, Webster GJM et al. Infection and hemostasis in decompensated cirrhosis: a prospective study using thrombolastrography. Hepatology 1999; 29: 1085-91.
FIGURE 1.
Correlation of F II and AT III values in patients group: r = 0,604,
y = 0,239 + 0,665x
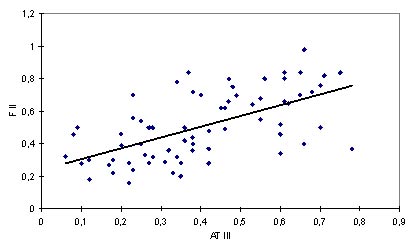
FIGURE 2.
Correlation of F V i AT III values in group of patients: r = 0,537,
y = 0,257 +
0,703x
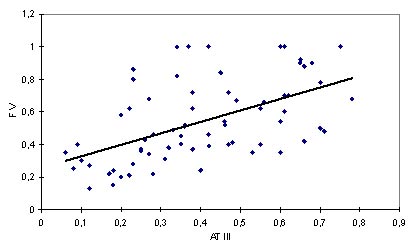
FIGURE 3. Correlation of F VII i AT III values in
patients group: r = 0,526,
y = 0,211 +
0,716x
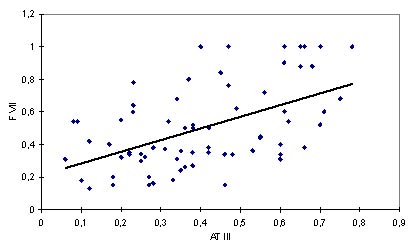
Table 1. Causes od bleeding in 69 patients with decompensated liver cirrhosis
|
CAUSE OF BLEEDING |
NUMBER (%) |
|
Oesophageal varices rupture |
16(73%) |
|
Ulcer, hypertensive gastropathy |
2(9%) |
|
Skin, urogenital tract |
2(9%) |
|
Bleeding in CNS |
1(4,5%) |
|
DIC |
1(4,5%) |
|
Total |
22(100%) |
Tabela 2. Causes of death in patients with
decompensated liver cirrhosis
|
CAUSE OF DEATH |
N |
% |
|
GI bleeding + coma |
12 |
41 |
|
Coma |
8 |
28 |
|
GI bleeding + shock |
3 |
10 |
|
Cardiovascular complications |
3 |
10 |
|
Unknown cause |
2 |
7 |
|
Infection |
1 |
4 |
|
Total |
29 |
100 |
Table 3. Values
of coagulation factors and inhibitor AT III
in control group and group of patients with decompensated liver cirrhosis
|
Factor |
Srednja vrednost (± SD) faktora |
t |
p |
|
|
control group N=30 |
patients N=69 |
|||
|
F II |
1,06 ± 0,14 |
0,51 ± 0,21 |
13,29 |
< 0,001 |
|
F V |
1,07 ± 0,12 |
0,54 ± 0,25 |
11,21 |
< 0,001 |
|
F VII |
1,04 ± 0,12 |
0,50 ± 0,26 |
11,05 |
< 0,001 |
|
AT III |
1,07 ± 0,16 |
0,40 ± 0,19 |
17,29 |
< 0,001 |
Table 4. Values
of coagulation factors and inhibitor AT
III in onset of bleeding
|
Factor |
MEan value (± SD) |
t |
p |
|
|
bleeding-no N=47 |
bleeding-yes N=47 |
|||
|
F II |
0,53 ± 0,22 |
0,47 ± 0,18 |
1,119 |
> 0,05 |
|
F V |
0,56 ± 0,25 |
0,49 ± 0,23 |
1,046 |
> 0,05 |
|
F VII |
0,52 ± 0,25 |
0,45 ± 0,27 |
1,119 |
> 0,05 |
|
AT III |
0,42 ± 0,20 |
0,36 ± 0,16 |
1,439 |
> 0,05 |
Tabela 5. Values
of coagulation factors and inhibitor AT
III in survival
|
factor |
Mean value (± SD) |
t |
p |
|
|
survived N=40 |
died N=29 |
|||
|
F II |
0,52 ± 0,22 |
0,48 ± 0,18 |
0,789 |
> 0,05 |
|
F V |
0,57 ± 0,25 |
0,50 ± 0,24 |
1,116 |
> 0,05 |
|
F VII |
0,49 ± 0,27 |
0,51 ± 0,24 |
0,405 |
> 0,05 |
|
AT III |
0,45 ± 0,19 |
0,34 ± 0,17 |
2,322 |
< 0,05 |
Tabela 6. Values
of coagulation factors and inhibitor AT
III in onset of bleeding and survival
|
factor |
bleeding |
F |
p |
|||
|
no |
yes |
|||||
|
survival |
survival |
|||||
|
yes (N=29) |
no (N=18) |
yes (N=11) |
no (N=11) |
|||
|
F II |
0,55 ± 0,23 |
0,49 ± 0,18 |
0,45 ± 0,19 |
0,48 ± 0,19 |
0,766 |
> 0,05 |
|
F V |
0,61 ± 0,26 |
0,49 ± 0,24 |
0,47 ± 0,20 |
0,52 ± 0,26 |
1,361 |
> 0,05 |
|
F VII |
0,53 ± 0,27 |
0,52 ± 0,22 |
0,39 ± 0,26 |
0,51 ± 0,28 |
0,858 |
> 0,05 |
|
AT III |
0,47 ± 0,20 |
0,36 ± 0,18 |
0,39 ± 0,16 |
0,32 ± 0,15 |
2,314 |
> 0,05 |