Gastroenterohepatologic iconography
Gastroenterohepatoloska ikonografija
ARCH GASTROENTEROHEPATOL
2002; 21 ( No 1 – 2 )
EOSINOPHILIC ASCITES
Eozinofilni ascites
1Mira Petrovic1 Vojislav N. Perisic, 2 Miodrag N.
Krstic, 3 Dejan Opric, 1 Sasa Milicevic.
( accepted May 20th, 2002 )
1 University Children , s Hospital, Belgrade,
2 Clinic for Gastroenterohepatology, Institute of Digestive Diseases,
Clinical Center of Serbia, Belgrade,
3Institute of Pathology, School of Medicine, University of Belgrade.
Address correspondent to: Professor Dr VN.Perisic
University Children, s Hospital
10 Tirsova St.
Yu-11000 Belgrade,
Serbia, Yugoslavia
………………………………………………………………………………………………
A 14-year old by was referred for further evaluation of his tense ascites and dull abdominal pain. This child developed insidious but progressive abdominal distension accompanied with dull abdominal pain few weeks before admission. He had past medical history of well-controlled bronchial asthma.
At admission,
beside tense ascitic peritoneal fluid effusion this patient, s
clinical finding was normal. Blood pressure was normal. Immediately performed
chest x – ray and ECG were normal as well. Laboratory investigations
demonstrated haematological abnormality of pronounced eosinophilia. Total white
blood cell count was 17.1 with increased number of eosinophils (20%, total
number 3400; normal < 500). ESR, hemoglobin, RBC, and trombocyte counts were
within reference range. Urinalysis was negative. Stools for ova and parasites
were
…………………….
…………………………………………..
Eosinophilic
ascites
Gastroenteroloska sekcija SLD-
01731, 2002.
repeatedly
negative. Blood biochemistry including blood sugar, BUN, serum creatinine,
liver function tests, total serum proteins, albumin, serum electrolytes, serum
and urinary amylases, and serum lipase were normal. IgA, IgM, and IgG were
within normal limits. Serum IgE was increased 800 u/ml (normal: 0-200).
Abdominal ultrasound scan revealed normal liver, spleen, and kidneys. No
abdominal masses were detected. Ascitic fluid effusion with floating small
bowel loops was seen. FIGURE 1. Diagnostic abdominal
paracentesis
was performed. Twenty milliliters of clear ascitic fluid was removed.
Its
biochemistry including glucose concentrations and amylase titer was normal
except protein concentration of 3.5g/l. After centrifugation, microscopic
examination of ascitic fluid sediment was made. Eight thousand cells,
exclusively eosinophils per 1 ml of ascitic fluid were found. FIGURE 2.
Two weeks of
methyl prednisolone treatment (30mg/day) led to quick and full amelioration of
peritoneal effusion which almost disappeared, normalisation of peripheral blood
eosinophilia, and reduction of serum IgE (350 u/ml). Six-month follow up was
uneventful, no peritoneal effusion recurred, and peripheral blood eospnophil
count was normal. Abdominal ultrasound examination was normal.
Comment: Eosinophilic gastroenteropathy may be protein
sensitive and idiopathic. Protein-sensitive forms of eosinophilic
gastroenteropathy occur in infants and children below the age of 2 years and
most commonly result from allergic reaction to cow , s milk or soy
protein or, infrequently, breast milk (1).
The idiopathic form presents with a highly variable clinical picture,
depending on the anatomic and histologic distribution of the eosinophilic
tissue infiltration. Tissue eosinophilia can be mucosal, muscular, or serosal
and has been described to affect the oeosphagus, stomach, intestine, or colon
alone or in combination (2).
The most
commonly encountered presentation results from mucosal involvement of the small
intestine and stomach (1,2,3). This usually presents with chronic diarrhoea
weight loss, malabsorption, and protein loosing enteropathy when small
intestinal mucosal infiltration with eosinophils occur. Eosinophilic gastritis
presents with epigastric pain, nausea, and vomiting.
Patients with
predominant muscle layer disease (eosinophilic infiltration of tunica
muscularis) manifest with pyloric, intestinal obstruction, or/and
achalasia-like picture (1,2,3).
The rarest
form is serosal layer disease, which typically present with eosinophilic
ascites (4). Serosal eosinophilic infiltration led to weeping of fluid in the
peritoneal cavity. An associated pleural effusion may be present. The fluid is
usually a sterile exudate that contains a high eosinophil count.
In
eosinophilic gastroenteropathy laboratory studies usually indicate peripheral
eosinophilia and increased serum IgE, particularly in children. In all cases,
stool studies must be done to rule out parasitic infestation. The radiographic
changes are found in mucosal and muscle layer disease. This are enlarged
gastric mucosal folds, pronounced antral and corporal nodularity, small
intestinal thickening of the folds with or without nodules (3). The small
intestine is dilated. Antro-pyloric obstruction, segmental small intestinal
obstruction, and achlasia-like x-ray picture are signs of muscle layer disease.
In serosal disease abdominal ultrasound demonstrates peritoneal effusion.
Endoscopic mucosal biopsies, laparoscopic muscle layer and serosal biopsies
indicating pure tissue eosinophilic infiltration and abdominal paracentesis
with cytology are important diagnostic methods.
Steroids are
the mainstay of therapy in particular in obstructive symptoms and eosinophilic
ascites. This disease tends to respond quickly. Occasionally low dose
maintenance steroids are needed to keep symptoms under control. In severe disease
additional immunosuppressive therapy using cyclosporine, azathioprine and
cyclophosphamide may be considered

Figure 1. Note Peritoneal effusion. Aspiration needle is visible
(arrow).
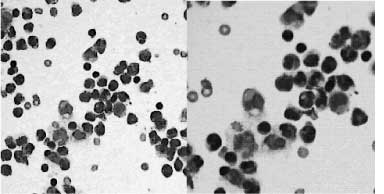
Figure 1. Eosinophilis in the ascitic fluid
REFERENCES:
1.Proujansky
R. Eosinophlic gastroenteritis. In: Pediatric gastrointestinal disease, Wyllie
R, Hyams JS, eds. Philadelphia: WB Saunders, 1993;566-71.
2.Steffen RM,
Wylie R, Petras RE, et al. The spectrum of eosinophilic gastroenteritis. Report
of six pediatric cases and review of the literature. Clin Ped 1991; 30: 404-11.
3.Talley NJ.
Eosinophilic gastroenteritis. In: Sleisenger and Fordtran, s
Gastrointestinal and liver disease, Feldman M, Scharschmidt BF, Sleisenger M,
eds. Philadelphia: WB Saunders, 1998; 1679-88.
4.Talley NJ,
Shorter RG, Philips SF, et al. Eosinophilic gastroenteritis. A
clinicopathological study of patients with disease of the mucosae, muscle
layer, and subserosal tissue. Gut 1990; 299-303.