Alimentary
tract and pancreas
Alimentarni
trakt i pankreas
ARCH GASTROENTEROHEPATOL 2002; 21 ( No 1 – 2
):
Endoscopic ultrasonoghraphy in Menetrier ’s
disease: A case report
Endoskopska ultrasonorafija u Menetrijerovoj bolesti: Prikaz slucaja
(
accepted February 10th, 2002 )
1Miodrag
Krstić, 2Gradimir Golubović, 1Marijan Micev, 1
Predrag Dugalić, 1Dragan Tomić, 1Aleksandra Pavlović.
1Institute
of Digestive Diseases, Clinical Center of Serbia, Belgrade,
2Department
of Internal Medicine. Clinical Hospital Zemun, Belgrade.
Abbreviations
used in this article: :
LGF,
large gastric folds; EUS, endoscopic ultrasound.
Addres
correspondence to: Docent Dr Miodrag N. Krstic,
Institute
of Digestive Diseases,
Clinical Center of Serbia,
6
Koste Todorovica St, YU-11000 Belgrade
Serbia,
Yugoslavia
E-mail:
[email protected]
………………
----------------------------
EUS
in Menetrier , s disease
Gastroenteroloska sekcija SLD-
01730, 2002.
ABSTRACT
The evaluation of patients with giant gastric rugal folds presents many problems to the gastroenterologist and pathologist. The variety of benign and malignant diseases must be considered in the differential diagnosis and all of them are difficult to separate by means of endoscopy and even biopsy. The unique ability of endoscopic ultrasound ( EUS ) to visualize the all layers of the gut wall makes it very useful in assessing patients with large gastric folds. EUS can precisely define which layers are thickened, characterise the echo pattern of thickness and whether the layer structure is preserved.
Menetrier’s disease is a prototype disease wich
caracterises deep mucosal thickening which can be clearly delineated by EUS. Here, we report the very first case of Menetrier’s disease which was
assessed by EUS in our country. The role of EUS in differential diagnosis of
large gastric folds is discussed in detail.
Key
words: Menetrier’s disease,
large gastric folds, EUS.
SAŽETAK
Evaluacija pacijenata sa
uvećanim želudačnim naborima je teška i za gastroenterologe i za
patologe. Veliki broj benignih i
malignih stanja mora da se uzeme u razmatranje dok endoskopija, pa čak i biopsija
najčešće ne mogu da napravi razliku izmedju njih. Endoskopski ultrazvuk je
posebno precizan u prikazivanjui slojeva zida digestivnog trakta te se stoga se
veoma uspešno koristi u ispitivanju pacijenata sa velikim želudačnim naborima.
On može jasno da ukaže koji sloj je zadebljao, kakva je ehogenost zadebljanja i
postoji li očuvan kontinuitet slojeva zida.
Menetrierova bolest je tipičan predstavnik
ove grupe obolenja i ona se odlikuje značajnim
zadebljanjem dubokog dela mukoze koje se jasno prikazuje na
endosonogafiji. U radu je prikazan prvi pacijent sa Menetrierovom bolešću koji
je u našoj zemlji analiziran endoskopskim ultrazvukom. U radu je takodje
detaljno diskutovana uloga EUS-a u diferencijalnoj dijagnozi uvećanih nabora želuca.
Kljucne
reci: Menetrierova
bolest, uvećani želudačni nabori, endoskopska ultrasonografija.

Figure
1. Menetrier disease – endoscopic view of large gastric folds
In body
and fundus
INTRODUCTION
The evaluation of the patients with giant
gastric mucosal usually imposes many problems to the gastroenterologist, the
pathologist and even surgeons (1). A
large scale of benign and malignant diseases should be considered in the
differential diagnosis (2). Standard endoscopic biopsy is oftenly superficial
for adequate histological diagnosis. The unique ability of endoscopic
ultrasound to visualize the layers of the gut wall makes it very useful in assessing
such patients (3).
Menetrier's disease is a prototype disease
in this category with typical thickening of deep mucosa (4). Here, we report a EUS finding in a patients
with Menetrier's disease.
CASE
REPORT
A middle aged man with Menetrier's disease
was refeered from Clinical Hospital Zemun for EUS assessment in October 1999.
The diagnosis of Menetrier's disease was established on previous
hospitalization a couple of months ago.
He had typical symptoms: profound weght loss, anorexia, voliting, diarrhoea
as well as symetric edema on legs. Biochemical blood tests disclosed
iron-defficiency anemia and marked hypoalbuminemia (<25g/l). On endoscopy,
the giant mucosal folds (>10mm) were observed in the stomach body and
fundus. Figure 1. Histology
disclosed foveolar hyperplasia and glandular atrophy without inflammation in
lamina propria mucosae. Figure 4.
Thus, the diagnosis of advanced Menetrier's disease was confirmed on the basis
of typical clinical, laboratory, endoscopical and histology findings.
On EUS, extended and diffuse thickening of
the second layer corresponding to deep mucosa was clearly demonstrated. Figure 2,3. A strict preservation of
five layer pattern of gastric wall was observed, too. The depth of 3rd
(submucosal) and 4th (muscle) layers was
not changed. The thickeness of 2nd layer was inhomogenous and more
hyperechoic.
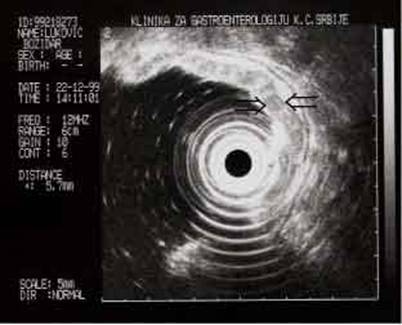
Figure 2. EUS Menetrier – thickening of II layer corresponding
to deep mucosa.
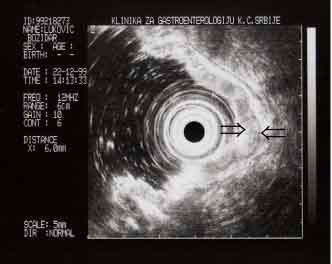
Figure 3. EUS Menetrier – thickening of deep mucosa with unchanged
submucosa and muscularis propria
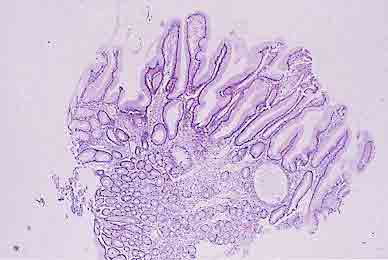
Figure 4. Menetrier disease. Hystology show marked fovelar
semicystic hyperplasia of deep mucosa (lamina propria mucosae)
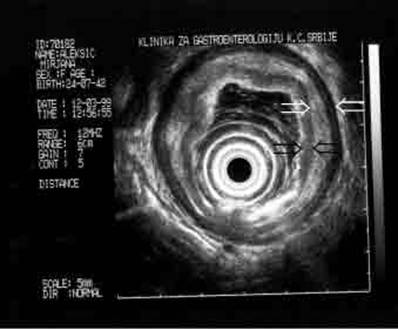
Figure 5. EUS in linitis plastica: uniform thickening of mucosa, submucosa and
muscularis propria: hypoechoic lamina propria mucosae between black arroeheds:
submucosa and muscularis propriabetween white arrowheds.
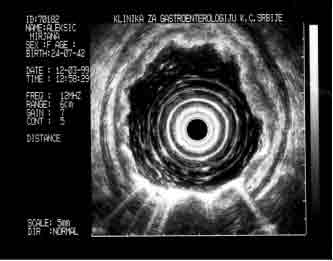
Figure 6. EUS in linitis plastica: Thickening of whole gut
wall
DISCUSSION
A broad spectrum of malignant and benign
stomach diseases may clinically and endoscopically present with giant mucosal
folds (1-7). Table 1. Barium X ray studies, CT, MR are of no value in differential diagnosis
of this condition. In the majority of cases endoscopic biopsies are not
sensitive enough (3). Full-thickeness
surgical biopsy used to be the golden
standard for diagnosis in past decades.
However, EUS is highly accurate in
visualisation of the gut wall (3) Echo-endoscopes with 12MHz transducers allows
demonstration of the 5-layer gut wall structue which almost completely
correlates with anatomic layers of the normal gut wall (I and II layer belongs
to the mucosa; III layer ressembles submucosa, IV muscularis propria and V is
adventitia or serosa). EUS can accurately disclose the disruption in the
continuity of the normal layer pattern which is invariably observed in
malignant diseases (4,5). EUS can also
determine with high sensitivity
which layers are thickened as
well as ECHO pattern of such enlargement (6).
Infiltrative gastric neoplasms, such as lymphoma or linitis plastica
type carcinoma produce diffuse thickening of all layers (6). Figure
5,6. Thus, EUS can facilitate the
differentation of benign from malignant aetiololgies (1-6).
Recent studies confirmed this statement
(7-10) Diffuse thickening of all layers or significant enlargement of 4th layer
(muscularis propria) was recorded only in malignant conditions (7). Diffuse
enlargement of 3 and 4 layer (submucosa
and muscularis propria) was present in patients with scihirrous carcinoma
(7,8). On the other hand, malignancy did not develop in all patients with
gastric wall thickening limited to layer 2 (deep mucosa) during a mean
follow-up period of 35 months (8). When the second layer alone is thickened,
Menetrier's disease should be at first considered as possible diagnosis and
when third layer alone is abnormally enlarged, anisakiasis might be suspected
(8). However, 2 and 3 layer enlargement may be present in healthy subjects with
hyperrugosity, but also in patients with lymphoma (8,9). In all malignant
conditions, thickening of the second layer was hypoechoic, too (1-9).
EUS finding in our patient was typical:
isolated, predominantly hyperechoic enlargement of second layer (deep mucosa)
with preservation of 5-layer wall structure. These features strongly suggested
benign aetiology of giant gastric folds, accoridng to the literature data (4-9).
On the other hand, EUS finding in Menetrier's disease, although typical is not
pathognomonic and diagnosis cannot be made with certainity without histology
(8-10). Histologic hallmark of diagnosis is marked elongation and turtuosity of
the pits (foveolar hyperplasia), accompanied by a reduction in the number of
oxyntric glands. Lamina propria is markedly edematous as well (10). Endoscopic
biopsy may not sample the full thickness of the mucosa thus revealing only the
foveolar hyperplasia. This is suggestive of diagnosis, but does not prove it
(10).
Typical EUS finding in conjuction with
foveolar hyperplasia on biopsy diminish the need for surgical biopsy (10). It can provide reassurance that
Menetrier's disease is likely or at least that thickened folds are benign (10).
In our case this was confirmed too.
REFERENCES:
1.Yasuda K. High-resolution endoluminal sonography of the upper gastrointestinal tract: The radial scanning ultrasound probe. Part II. In: Van Dam J, Sivak MV. Gastrointestinal endosonography. Philadelphia: W.B.Saunders; 1999;95-100.
2.Yasuda K. The handbook of endoscopic ultrasonography in digestive tract. Ied. Oxford.: Blackwell Science; 2000.
3.Dancygier H, Lightdale C, Stevens P.Endoscopic ultrasonography of the upper gastrointestinal tract and colon. In: Dancygier H, Lightdale J. Endosonography in gastroenterology Ied. Stuttgart-New York: Thieme-Verlag; 1999; 13-174.
4. Michael B. Kimmey, Peter Vilmann: Endoscopic ultrasonography In. Yamada, et al: Textbook of gastroenterology VIed. Philadelphia : Lippnicott Wiliams and Wilkins; 1999; Chapter 136.
5. Carletti G, Fusaroli P, Bocus P. Endoscopic Ultrasonography. Digestion 1998; 59: 509-530.
6. Chak A. Endoscopic Ultrasonography. Endoscopy 2000; 32: 146-152
7.
Mendis
RE, Gerdes H, Lightdale C, et al. Large gastric folds: a diagnostic approach
using endoscopic ultrasonography. Gastrointestinal Endosc 1994;40:437-441.
8.
Songur
Y, Okai T, Watanabe H, et al. Endosonographic evaluation of giant gastric
folds. Gastrointestinal Endos 1995; 41: 468-474.
9.
Manuory
V, Klein O, Houcke ML, et al. Endoscopic ultrasonography in the diagnosis of
hypertrophic gastropathy (letter). Gastroenterology 1994; 106:820.
10.
Okuda
M, Iiyuka Y, Oh K, et al. Gastritis cystica profunda presenting as giant
gastric mucosal folds. The role of endoscopic ultrasonography and mucosectomy
in the diagnostic work up. Gastrointestinal Endosc 1994; 40: 640-44.
|
BENIGN DISEASES |
MALIGNANT DISEASES |
|
Menetrier's disease |
Carcinoma |
|
Zollinger-Ellison syndrome |
Lymphoma |
|
Lymphocytic and Eosinophylic gastritis |
Lymphoma of MALT |
|
Normal hyperrugosity |
Carcinoid |
|
Sarcoidoses and amyloidoses |
|
|
Crohn's disease |
|
|
TB and syphilis |
|
|
H.pyloris; CMV and H.simplex virus |
|
Table 1. Classification of large gastric folds.