Hematochezia due to short - gut colitis
Hematohezija prouzrokovana kolitisom kratkog creva
(accepted June 30¸ 1999)
Address correspondence to:
Professor Dr VN.Perisic¸
University Children's Hospital,
Tirsova 10 Str,
YU - 11000 Belgrade, Yugoslavia,
FAX ( 381 11 ) 684 672
Sazetak
U radu se prikazuje dete sa produzenim tokom rektalnog krvarenja prouzrokovanog neuobicajenom vrstom kolitisa: kolitisom kratkog creva. Pacijent je bilo novorodjeno dete sa atrezijom ileuma koje je operisano neposredno posle rodjenja. Dve nedelje posle uspostavljenog oralnog unosa mleka doslo je do rektalnog krvarenja i teske anemija prouzrokovane hemoragijskim kolitisom koji se poboljsao primenom hidrokortizonskih klizmi i sulfasalazina. Kolitis kratkog creva je jos jedan neuobicajeni oblik kolitisa koji moze da se ispolji iskljucivo rektalnim krvarenjem.
Kljucne reci: kratko crevo¸ hematohezija¸ kolitis.
Abstract
We present a case history of the child with protracted course of rectal bleeding due to unusual form of colitis: short-gut colitis. The child was an infant with ileal atresia who was successfuly operated immediately after birth. Two weeks after enteral feeding was introduced he developed rectal bleeding and severe anemia due to haemorrhagic colitis which gradually improved on hydrocortisone enema and with sulfasalazine. Short-gut colitis is another unusual colitis which may present exclusively with rectal bleeding.
Key Words: short-gut¸ hematochezia¸ colitis.
Abreviations used in this article:
IBD, inflammatory bowel disease;
TPN, total parenteral nutrition.
INTRODUCTION
Over the last decade several new forms of IBD have been described (1). Some may present with rectal bleeding, e.g. allergic colitis (2,3). There is also evidence that during advancement of enteral feeding some infants with short - gut syndrome may experience non - infectious colitis associated with hematochezia: namely short - gut colitis (4). Although non - specific, endoscopic findings and mucosal histology were similar in all cases (4). Rectal bleeding was improved most effectively when predigested milk formula feeding was stopped and / or sulfasalazine was administered (4). This type of colitis was thought unliklely to be of allergic in nature (4). Here¸ we report the child with short - gut syndrome who presented exclusively with pronounced rectal bleeding.
CASE REPORT
A 55 - day old malnourished and anaemic boy had a 27 -day history of severe haemorrhagic diarrhoea. The infant was the first child of healthy ulrelated parents. The pregnancy and delivery were normal. At 5th month of ggth of gestation he was diagnosed as having distal small bowel obstruction by ultrasound. Eighteen hours after delivery an exploratory laparotomy was performed. Multiple ileal atresias were found and an extensive intestinal resection preserving ileocaecal valve and 7cm of terminal ileum was performed. Residual small bowel lenght was not measured but it was presumed to be short. Postoperative recovery was uneventful. Ten days TPN was followed by oral feeding with l / 4 strenght hydrolyzed casein formula (Pregestimil, Mead Johnson). Bloody diarrhoea developed 2 weeks after formula feeding¸ when full strenght milk was inroduced. The boy gradually lost weight. On addmision to our department his weight was 3500gr (birth weight 3400 gr), lenght 50cm. Beside the signs of malnutrition and pallor his findings were otherwise normal. Laboratory investigations showed hemoglobin concentration 82 g/L, RBC 2.87 x 1012/L, Hct 25.3%, WBC 10.3 x 109 / L, Plt 424 x 109 /L, Urinalysis was normal. Total serum protein concentration was 54 g / L, and serum albumin 30 g / L.
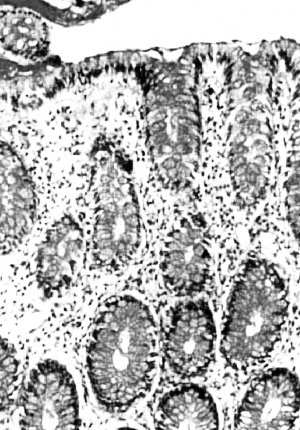
Serum electrolytes, BUN, blood sugar, liver function tests including PT and PTT were normal. Repeated stool cultures were negative. Milk dilution regrading did not improve the infant's diarrhoea. Flexible sigmoidoscopy revealed moderate to severe mucosal oedema and hyperemia, and very pronounced mucosal friability. Colonic biopsy specimens demonstrated marked oedema, mixed inflammatory infiltrate of lamina propria, and significantly increased number of esinophils. Crypt architecture was preserved. Packed red blood cells, 20% albumin, and plasma transfusions were given. Cholestyramine 250 mg / kg / 24h reduced stool frequency but failed to control rectal bleeding. Ten days daily hydrocortisone enema pne enema promptly abated infant's diarrhoeal illnness and rectal bleeding. Oral administration of mesalazine (25 mg / kg / 24h) was followed by haemorrhagic diarrhoea. On the contrary, sulfasalazine therapy 40 mg / kg / 24h led to full resolution of bloody diaaa diarrhoea and tolerance of full strenght formula feeding. One month infant's weight gain was 710 gr. Four month course of sulfasalazine maintained this boy in full clinical remission, and enabled him to develop properly. Thereafter, sulfasalazine withdrawl did not elict a recurrence of rectal haemorrhage. Boy continued to developproperely without any disease symptom.
DISCUSSION
Colitis in infancy and childhood encompass a heterogenous group of illnesses (1, 3, 5,6). Infective colitides, allergic colitis and ulcerative colitis may all cause severe rectal haemorrhage (1,3,7). In contrast, newly recognised forms of colitis, e.g.collagenous, and microcosopic (lymphocytic), usually present with chronic watery diarrhoea (8, 9, 10). We further showed that short - gut colitis may occur in up to 80% of infants with short bowel syndrome (4). Although all patients responded more or less well to predigested formula withdrawal, there was no evidence that this new form of colitis is allergic in nature (4). We found that sulfasalazine treatment enabled an infant to resume full enteral feeding without further bleeding. (4). We demonstrated that full strenght Pregestimil formula was tolerated only when sulfasalazine was given. Mesalazine treatment in contrast¸ failed to control colonic haemorrhages. This observation further supports the concept of the importance of both sulfasalazine components, sulfapyridine and 5 - aminosalicylic acid. Possible antibacterial action of sulfapyridine on colonic flora may play some role since short - gut colitis may be partly contributed by excessive production of short - chain fatty acids by colonic bacteria due to proximally malabsored carbohydrates (4,11). In short - gut colitis sulfasalazine improves predigested formula tolerance enabling advancements in enteral feeding and subsequent improvement of intestinal adaptation (4). This drug has to be given temporalily until stable and prolonged full enteral feeding, and nutritional recovery occur. In conclusion, short - gut colitis is rare form of paediatric colitis which may present with rectal bleeding. Endoscopic findings, musocal histology, and reponse to sulfasalasine classify this colitis as new member of IBD group.
REFERENCES:
1. Booth IW. Chronic inflammatory bowel disease. Arch Dis Child 1991; 66: 742 - 4.
2. Dupont C, Badoual J, Le Luyer, e Bourgeois C, Barbet J - P, Voyer M. Rectosigmoidoscopic findings during isolated rectal bleeding in the neonate. J Pediatr GLe Bourgeois C, Barbet J - P, Voyer M. Rectosigmoidoscopic findings during isolated rectal bleeding in the neonate. J Pediatr Gastroenterol Nutr 1987; 6: 257 - 4.
3. Perisic VN, Filipovic D, Kokai G. Allergic colitis with rectal bleeding in an exclusively breast - fed neonate. Acta Paediatr Scand 1988; 77: 163 - 4.
4. Taylor SF, Sondheimer JM, Sokol RJ, Silverman A, Eilson HL. Noninfectious colitis associated with short gut syndrome in infants. J Pediatr 1991; 119: 24 - 8.
5. Sanderson IR. Unusual colitides. Balliere's Clin Gastroenterol 1994, 8 181 - 96.
6. Ojuawo A, St Lous D, Lindley KJ, Milla PJ. Non - infective colitis in infancy an evidence in favor of minor immunodeficiency in its pathogenesis. Arch Dis Child 1997, 76 345 - 8.
7. Gryboski JD. Ulcerative colitis in children 10 years and younger. J Pediatr Gastroenterol Nutr 1993, 17 24 - 31.
8. Bogomoletz WV, Flejou JF. Newly recognized forms of colitis: collagenous colitis, microscopic ( lymphocytic ) colitis, and lymphoid follicular proctitis. Sem Diagn Path 1991; 8: 178 - 89.
9. Perisic VN, Kokai GK. Diarrhoea caused by collagenous colitis. Arch Dis Child 1989, 64 867 - 8.
10. Sanderson IR, Boyle S, Williams CB, Walker - Smith JA. Histological abnormalities in biopsies from macroscopically normal colonoscopies. Arch Dis Child 1986, 61 264 - 7.
11. Vernia P, Caprilli R, Latella G, Barbetti F, Magliocca FM, Cittadini M. Fecal lactate and ulcerative colitis. Gastroenterology, 95 1564 - 8.