Neda SVIRTLIH
Institute for Infectious and Tropical Diseases Medical Faculty University of Belgrade, Clinical Centre of Serbia, Belgrade
Address correspondence to Assistant Prof Neda Svirtlih, MD, PhD, Institute for Infectious Diseases Medical Faculty University of Belgrade, Bul JNA 16, 11000 Belgrade, Serbia, Yugoslavia
phone: 381-11-68-40-71; Fax: 381-11-68-42-72; e-mail: [email protected]
ABBREVATIONS: DNA- deoxiribonucleid acid; HAV- hepatitis A virus; HBV- hepatitis B virus; HCV- hepatitis C virus; HEV- hepatitis E virus; HIV- human immunodeficiency virus; ORF- open reading frame; PTH- posttransfusion hepatitis; PCR- polymerase chain reaction; TTV- TT virus
ABSTRACT
TT virus (TTV) is discovered at the end of 1997 as a human DNA virus by Japanese authors in patients with posttransfusion hepatitis of unknown etiology. Investigations of the virus throughout the world demonstrated its high prevalence, particularly in some geographic reagions. For example, in Japan, the prevalence ratio is found up to 92%, 62,5% and 60% in healthy controls, chronic cryptogenic hepatitis and "idiopathic" acute hepatitis, respectively. In USA and European countries, the prevalence of TTV is lower.The diagnosis of the virus is based on an amplification methodology of the genome, using polimerase chain reaction. The virus itself has high genome diversities what could be a possible reason for his long persistence. The results of investigations of the viral pathogenicity and its role in liver disease, are still conflicting. According to data, it seems that this virus is a relative attractive candidate virus as a potential etiologic factor for acute and chronic hepatitis and liver malignancy.
SAZETAK
TT virus je humani DNK virus koji je otkriven krajem l997 godine u krvi bolesnika obolelih od posttransfuzionog hepatitisa nepoznate etiologije. Opisan je od strane japanskih istrazivaca. Ispitivanja prevalence virusa sirom sveta pokazalo je njegovu visoku prevalencu, posebno u nekim delovima. Na primer, u Japanu je nadjeno da je njegova prevalenca cak do 92% u zdravih ljudi, zatim do 62,5% u osoba sa hronicnim i u do 60% osoba sa akutnim hepatitisom nepoznate etiologije. U SAD i Evropskim zemljama, prevalenca ovog virusa je znatno manja. Dijagnoza TT virusa za sada se vrsi pomocu umnozavanja njegovog genoma. Sam virus ispoljava siroku gensku sarolikost sto je verovatno razlog njegovom visegodisnjem odrzavanju. Rezultati istrazivanja patogenosti virusa i njegovog udela u bolesti jetre, jos uvek su razliciti. Prema dosadasnjim podacima, TT virus nije znacajan etioloski faktor u akutnom ili hronicnom hepatitisu pa ni u nastanku maligniteta jetre.
KEY WORDS: TT virus, liver disease
INTRODUCTION
TT virus (TTV) was identified by Nishizawa at al. in sera samples from Japanes patients and the discovery was published in the literature at the end of 1997 (1). The virus was named with the initials of the person in whose serum it was first detected (patient T.T.). This virus was described as a novel virus which caused acute non A-G pottransfusion hepatitis (PTH). Namely, by means of polymerase chain reaction (PCR), the authors isolated and described the viral clone (N22) of 500 nucleotides with poor homology to any previously reported virus sequences in sera from 3 of 5 patients with PTH of unknown etiology. As this clone was sensitive to DNase, that confirmed that it was DNA virus. TTV DNA titers closely correlated with aminiotransferase levels in all three patients with PTH including the index case.
Subsequently, many studies from Japan as well as from many other countries were done in order to investigate the epidemiology, risk of transmission, possibillity of persistence and clinical significance of the novel virus and determine its role in liver disease. At the same time, different new techincs from molecular biology were perfomed to assess the genomic characteristics of the TTV. Until now, many of them are very conflicting and are still under evaluations. However, in this review article based on published references from the literature from 1997 through 1999, the author would like to present the results of different aspects of the novel virus with their disagrees and dilemas.
CHARACTERSTICS OF THE VIRUS AND ITS DIAGNOSIS
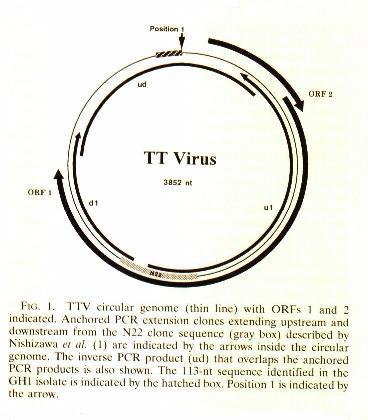
TT virus is an unenveloped virus size of 30-50 nm. Cesium cholride density gradient centrifugation bands of the virus at 1.31-1.34 g/ml (2,3). The molecular characterisation of the prototype TTV isolate (TA278) and other isolates, has shown that TTV was a circular and negative single-stranded DNA with 3852 nucleotides. It has two large overlapping open reading frames (ORFs), ORF1 and ORF2, (encoding 770 and 202 amino acids, correnspondingly) and several smalles (3,4). Nucleotide sequences of the coding regions are highly variable, while sequences of the noncoding region are conserved. The properties of TTV earlier suggested that it could belong to the Parvoviridae family. However, recent investigations showed that it did not have the terminal structure typical of a parvoviruses and did share some atributes of Circoviridae, the members wich include chicken anemia virus (CAV), psittacine beak virus, feather disease virus and porcine circovirus (3,5). Although the size of TTV particule and DNA genome are larger than Circoviridae, they possess similar densities, thus suggesting a similar protein DNA ratio. So, the distinct biophysical and molecular characteristics of TTV from known viruses, suggest that it is a member of a new family of viruses, tentatively named Circinoviridae (3,5). Also, intravenous inoculation of TTV-positive human serum into chimpanzees demonstrated that it could be transmitted to primates and detected in sera and feces, but no biochemical or histological evidences of hepatitis were observed (3).
TT virus has wide sequence divergences (approximately 52%), by which it is classified into at least l6 genotypes (types ), separated by an evolutionary distance of >0.30 (6). Genotypes are furher divided into subtypes (evolutary distance >0.15), making the phylogenetic tree of the virus which is stil under investigation (7,8,9). Under investigations are also a correlation of those types and subtypes with geographic distributions. However, data has shown that some individuals colud be infected with more than one genotype (10,11). That colud be intersting for viral persistence and potential clinical influence of its infection on liver disease (12).
At present, there is no sensitive and specific serological tests or in vitro culture for TTV. The diagnosis of the virus is based on DNA polymerase chain reaction ( PCR ) by amplification of the whole extracted genome or its particular sequences and sensitivity and specificity are highly influenced by used set primers. Depending of the sequence heterogenicity between different region of the virus, it is suggested that conserved sequences in the noncoding region could be used as primers for sensitivity for detecting TTV, while divergent sequences in noncoding region would be useful as primers for distinguishing various viral genotypes (4). Recently, a new fluorescent method for measuring the quantity of TTV DNA was developed which could detect the amount of the genome (13).
Use of PCR has demonstrated TTV in sera, liver tissue, peripheral blood mononuclear cells (PBMC), bile and feces (l4,l5,l6,l7,18). Detection of viral DNA in the liver and PBMC of infected subjects suggests that TTV is hepatotropic and possibly, that it could replicate in other cells exept hepatocytes. Also, such different sources of viral identification are improtant for virus loading and routes of infection.
EPIDEMIOLOGY OF TTV AND RISK OF TRANSMISSION
The world prevalence of TTV is very variable, mainly depending of the assay sensitivity and specificity. It includes the choice of the primer set for PCR diagnostic methodology, the procedure of PCR assay (e.g. nested or semi-nested) as well as of the part or whole genome for selection and amplification. As different primers could give different genome detection results, it may be the reason for great disproportions of reported results in epidemiology investigations.
The prevalence of TTV was first started to investigate in Japanese patients and then broadened to other countries throuhgout the world. TTV DNA was detected in heterogeneous individuals, from healthy people as were blood donors, then, in the patients with acute and chronic hepatitis of unknown etiology or coinfected with known viruses (mostly with hepatitis C virus infection), patients with a risk of parenteral infections (e.g. patients who received blood and blood products, i.v. drug users, patients with thalassemia and hemophilia, patients on hemodialysis), moreover, in the patients with high risk of sexual infections etc.
TTV DNA positivity was found in the rates from 5% to 92% in investigations from Japanese blood donors (19,20,21,22,23,24). In mostly reports, the TTV prevalences were higher than 20%, confirming earlier suspected assumption for precisely primers use in practical investigations. In different other healthy population, e.g. medical workers and pregnant women, detected rates of TTV DNA were 24% and 27,8%, respectively (25,26). The prevalence in children was lower than adults with the rate of 5% (27). According to those data, the prevalence of TTV in Japanese general population is obviously extremelly high.
On contrary, investigations in other world regions determinated the prevalence of TTV DNA in much lower rates. For example in USA, the prevalence in blood donors was found from 1% to 10% (28,29,30). Very similar, in European countries, TTV prevalence rates were found from 1.9% to 13.7% (11,31,32,33,34). Suprisingly, in a very resent report from Italian authors, in patients which were not selected and with different spectrum of diseases beside liver diseases, the averege prevalence of TTV was 50% using amplification of ORFl of the standard isolate TA 278 (35). Other investigastion reports from Brasil, Mongolia, Thailand ,Taiwan and Korea reported the prevalences of TTV DNA in 62%; 42,9%; 7%; 53% and 17,6%, respectively (36,37,38,39,40,41).
The prevalences of the virus in parenteraly infected risk group patients as are patients with multiple transfusions of blood and blood products and intravenous drug abusers, also are very conflicting. In US investigations, the authors concluded that patients with a history of prior exposure to blood products were associated with 4.2 time more increased risk of TTV infection than patients without that data (28). Similar results were reported from Spain, Thailand, UK and Japan and all of them emphazed improtance of parenteral infection for catching up the TT virus (31,38). Opposite to those results are results from other authors who did not confirmed any association between exposure to blood or association of sexual behavior and TT virus infection (30,31,41,42). Moreover, many authors reported that although that high prevalences of TTV DNA were detected in patients on hemodialysis, hemophiliacs, patients with thalassemia and bone marrow transplantation, no significant differences were noticed in prevalences between those patients and the prevalence in general populations (10,21,34,35,42,43). So it is evident that increased prevalence of TTV viremia in a risk groups for parenterally infection can only indicate that TTV is transmissible by parenteral route. But, lack of difference of frequencies between TTV viremia and risk groups patients, general population and other parenterally transmissible viruses (such as HBV, HCV and HIV) in some studies, is difficult to explain. Regardless to detection efficiency, low viral titre may be associated with reduced infectivity through blood, needle stick injures and sexual contacts and may be additional reasons for those unexpected findings.
In some sudies the authors presented results with different findings between circulating TTV DNA and strictly parenteral viruses eg. HCV an HBV and concluded that the main transmission of TTV could be differetnt that those viruses (28,42,45). Moreover, data with results that infection with TTV increases with age, also suggests that an alternative routes of transmission, as enterally, may exist (32,33,39). Detection of TTV in feces of some infected persons, isolation the same virus strain in blood and feces and low viral prevalence in developed countries, potentially provides a route of transmission comparable to enteroviruses, such are HAV and HEV (22,26,39,42,44). Also, reports with evidences that most children with TTV-negative mothers acquired infection at longer that 3-4 months postpartum, as well, that children were infected with different strains unrelated to strains of their TTV-positive mothers, support the possibility of viral enterically transmission (26,46). Finally, high prevalences of TTV in some countries as Japan, suggests that not only parenteral route of infection, but an enviromental source may be important for TTV epidemiology.
CLINICAL CHARACTERISTICS OF TTV INFECTION
The discovery of the novel TT virus and its high prevalences in some geographic areas, obligated for further investigations about its role in liver diseases. It was important first of all to investigate the prevalence of the TTV in different liver diseases of unknown etiology and/or coinfected with HCV and HBV. Large studies in last two years presented such results in order to establish the significance of the TTV as etiological factor in acute and chronic hepatitis as well as in hepatocelullar carcinoma. Most of that studies presented their results of circulating TTV DNA in a wide spectrum of clinical forms of liver diseases as comparison viral titar with aminotransferases values.
As it was been expected, the circulating of TTV DNA were more frequent in area with high prevalence of TTV. For example, in Japan, several studies demonstrated TTV DNA in chronic hepatitis and cirrhosis with unknown etiology in prevalences ranging between 12% and 62.5% (20,47,48). In acute non A-G hepatitis resembling viral etiology, authors from Japan reported TTV DNA prevalences from 29% to 60% (47,48,49). In other countries, prevalences of TTV DNA in liver diseases of unknown etiology were reported in a very wide rate of occurrence. In chronic cryptogenic hepatitis in USA, Korea, Thailand and Mongolia, the authors reported prevalences of l5%, l7.6%, l8% and 47%, respectively. In cases of idiopathic acute hepatitis, TTV DNA were reported from USA, Germany and Brasil in prevalences of 23,2%, 16% and 71%, respectively. Of special interest are reports from USA and Spain with prevalences of TTV DNA in idiopathic fulminant hepatic failure in 27% and 39,6% ( 28,31). Based on the obtained results, the correlation of the prevalence of TTV DNA in patients with acute and chronic idiopathic liver diseases and the prevalence of the virus in general population, it is not possible to point the significant role of the virus as etiological factor. Moreover, investigations of patients prior to liver transplantation from three groups of authors from Germany concluded that presence of TTV had not any influence to end stage of liver disease compared to other viruses (50,51,52). Reported studies about the association of hepatocelullar carcinoma and TT virus, also did not confirm the integration of the TTV genome into host genome or possible significance of the virus in developing malignancy of the liver (14,53).
More intriguing are investigations which are done between the correlation of the presence and titar of TTV DNA and aminotransferases levels what could be a possible contribution for evidence of eventually hepatocidal effect of the virus. In those reports, results and conclusions are conflicting, also. Some authors were able to find a significant correlation between aminotransferase levels and viral titar and so confirmed that TT virus could be a pathogen virus for the liver (56,57). Authors without same results leave us in dilema if it is strongly a hepatotropic virus or it only persists such as HGB-C virus does (29,31,37). Originally reported by Nishizawa et al., PTH in three patients were followed by elevated aminotransferase values and the novel virus was designated as etiological factor, but the fact was that those patients had carcinoma and had no any clinical singh of hepatitis.
Extending investigations in connection with clinical data, some authors explored the effect of intreferon therapy in patients with TT virus infection and also in patients with TTV coinfection with HCV. They reported no influence on interferon therapy in chronic cryptogenic hepatitis with TTV whether patients were infected or not with HCV as well as they did not find any influnece of TTV to therapy of chronic HCV infection (35,58).
Viral persistence was the particular object of investigation. Viral inconstancy with hypervariable regions and differetnt types and subtypes even in the same individuals, was responsible for acceptible hypothesis that TT virus had existed before it was discovered and that was comfirmed (10,59). Retrospectively, searching the virus in stored sera , in most patients virus persistence was detected from 3 to 6 years ( from 6 months to 22 yrs) (11,29,41,43).
At least, to determine the clinical manifestations and histopathologic features of TTV DNA-positive chronic liver disease in Japanese patients, several following characteristics were observed: biochemical abnormalities with elevated ALT and GGPT ensymes resembling fatty liver or alchoholic liver disfunction and well response to liver-protective medicines, inflamation cell infiltration scattered in portal area with distinguishable necroinflamation in the lobular region, pathologic findings on biliary epithelium, high incidence of steato-metamorphosis involment and histologic characteristics undistinguishable from "viral" chronic hepatitis in some liver specimens (60).
According to data from the literature, TT virus is newly discovered human DNA virus with obviously high prevalences in some geographic area. With great genetic diversity, the virus is capable to evade immune response and persists many years in the individuals. The route of transmission of the virus is certainly parenteral but another routes of infection can not be excluded. The virus repilicates in hepatocytes and some other cells of hematopoetic origins, made himself tropic for different human cells. If it is only tropic or is responsible to cause a clinically disease, remains to be determinated in the future. Since now, it is likely that TT virus is human, mostly hepatotropic "bystander" virus with no pathogenic effect.
REFERENCES:
1 - Nishizawa T, Okamoto H, Konishi K, Yoshizava H, Miyakawa Y, Mayumi M. A novel DNA virus (TTV) associated with elevated transaminase levels in posttransfusion hepatitis of unknown etiology. Biochem Biophys Res Commun 1997; 24 l (1): 92-7.
2 - Okamoto H. Molecular virology of TT virus. Nippon Rinsho 1999; 57 (6): 1239-49.
3 - Mushahwar IK, Erker JC, Muerhoff AS et al. Molecular and biophysical characterization of TT virus: Evidence for a new virus family infecting humans. Proc Natl Acad Sci USA 1999; 96 (6); 3177-82.
4 - Okamoto H, Nishizava T, Ukita M et al. The entire nucleotide sequence of TT virus isolate from the United States (TUS01): comparison with reported isolates and phylogenetic analysis. Virology 1999; 259 (2): 437-48.
5 - Miyata H, Tsunoda H, Kazi A et al. Identification of novel GC-rich 113-nucleotide region to complete the circular, single-straned DNA genome of TT virus, first human circovirus. J Virol 1999; 73 (5): 3582-6.
6 - Okamoto H, Takahashi M, Nishizawa Tet al. Marked genetic heterogeneity and frequent mixed infection of TT virus demonstrated by PCR with primers coding and noncoding regions. Virology 1999; 259 (2): 428-36.
7 - Viazov S, Ross RS, Niel C et al. Sequence variability in the putative coding region of TT virus: evidence for two rather than several major types. J Gen Virol 1998; 79 (12); 3085-9.
8 - Hijakata M, Takahashi M, Mishiro S. Complete circular DNA genome of a TT virus variant (Isolate name SANBAN) and 44 partial ORF2 sequences implicating a great degree of diversity beyond genotypes. Virology 1999; 260 (1): 17-22.
9 - Tanaka Y, Mizokami M, Orito E et al. A new genotype of TT virus (TTV) infection among Colombian native Indians. J Med Virol 1999; 57 (3): 264-8.
10 - Takayama S, Yamazaki S, Matsuo S, Sugii S. Multiple infection of TT virus (TTV) with different genotypes in Japanese hemophiliacs. Biochem Biophys Res Comm 1999; 256 (1): 208-11.
11 - Irving WL, Ball JK, Berridge S, Curran R, Grabowska AM. TT virus infection in patients with hepatitis C: frequency, persistence and sequence heterogeneity. J Infect Dis 1999; 180 (27): 27-34.
12 - Kurihara C, Ishiyama N, Nishiyama Y, Miura S. The association of TTV genetic variant with liver disease. Nippon Rinsho 1999; 57 (6): 1256-61.
13 - Kakinuma K, Yamauchi T, Hikiji K, Tsukada Y. Development the quantification method of TTV- DNA and clinical application. Nippon Rinsho 1999; 57 (6): 1262-4.
14 - Yamamoto T, Kajino K, Ogawa M et al. Hepatocellular carcinomas infected with the novel TT DNA virus lack viral integration. Biochem Biophys Res Commun 1998; 251 (1): 339-43.
15 - Okamura A, Yoshioka M, Kubota M, Kikuta H, Ishioko H, Kobayashi K. Detection of novel DNA virus (TTV) sequence in peripheral blood mononuclear cells. J Med Virol 1999; 58 (2): 174-7.
16 - Okamoto H, Kato N, Iizuka H, Tsuda F, Miyakawa Y, Mayumi M. Distinct genotypes of nonenveloped DNA virus associated with posttransfusion non-A to G hepatitis (TT virus) in plasma and blood mononuclear cells. J Med Virol 1999; 57 (3): 252-8.
17 - Okamoto H, Akahane U, Ukita M et al. Fecal extretion of nonenveloped DNA virus (TTV) associated with posttransfusion non-A-G hepatitis of unknown etiology. J Med Virol 1998; 56 (2): 128-39.
18 - Ukita M, Okamoto H, Kato N, Miyakawa Y, Mayumi M. Excretion into bile of novel unenveloped DNA virus (TT virus) associated with acute and chronic non-A-G hepatitis. J Infect Dis 1999; 179 (5): 1245-8.
19 - Hadama T, Takami S, Kinshita M. Detection of TT virus in healthy volunteer. Nippon Rinsho 1999; 57 (6): 1300-4.
20 - Chayama K. Detection of TT virus DNA in patients with non-A to G liver diseases. Nippon Rinsho 1999; 57 (6): 1295-9.
21 - Kanda Y, Tanaka Y, Kami M, Saito T, Asai T, Izutsu K et al. TT Virus in bone marrow transplant recipients. Blood 1999; 93 (8): 2485-90.
29 - Matsumoto A, Yeo AE, Shih JW, Tanaka E, Kiysawa K, Alter HJ. Transfusion-associated TT virus infection and its relationship to liver diseases. Hepatology 1999; 30 (1): 283-8.
30 - Desai SM, Muerhoff AS, Leary TR. Prevalence of TT virus in US blood donors and populations at risk for acquiring parenterally transmitted viruses. J Infect Dis 1999; 179 (5): 1242-4.
31 - Gimenez-Brakons M, Forns X, Ampurdanes S, Guilera M, Soler M, Soguero C et al. Infection with a novel human DNA virus (TTV) has no pathogenic significance in patients with liver diseases. J Hepatol 1999; 30 (6): 1028-35.
32 - MacDonald DM, Scott GR, Clutterbuck D, Simmonds P. Infrequent detection of TT virus infection in intravenous drug users, prostitutes and homosexual men. J Infect Dis 1999; 179 (3): 686-9.
33 - Simmnonds P, Davidson P, Lycett C, Prescott LE, MacDonald DM, Ellender J et al. Detection of novel DNA virus (TT virus) in blood doonors and blood products. Lancet 1998; 352 (9123): 191-5.
34 - Gallian P, Berland Y, Olmer M, Raccach D, de Micco P, Biagini Pet al. TT virus infection in French hemodialysis patients: study of prevalence and risk factor. J Clin Microbiol 1999; 37 (6): 2538-42.
35 - Maggi F, Fornai C, Morrica A, Casula F, Vatteroni AM, Ciccorossi P et al. High prevalence of TT virus viremia in Italian patients, regardless of age, clinical diagnosis and previous intreferon treatment. J Inf Dis 1999; 180 (3): 38-42.
36 - Niel C, de Oliveira J, Ross Rudolf, Gomes S, Roggendorf M, Viazov S. High prevalence of TT virus infection in Brazilian blood donors. J Med Virol 1999; 57 (3): 259-63.
37 - Kato H, Mizokami M, Nakano T, Kondo Y, Dashnyam B, Oyunsuren T et al. High prevalence and phylogenetic analysis of TT-virus infection in Mongolia. Virus Res 1999; 60 (2): 171-9.
38 - Poovorawan Y, Theamboonlers A, Jantaradsamee P, Kaew N, Hirsch P, Tangkitvanich P. Hepatitis TT virus infection in high-risk groups. Infection 1999; 26 (6): 355-8.
39 - Hsieh SY, Wu YH, Ho YP, Tsao KC, Yeh CT, Liaw YF. High prevalence of TT virus infection in healthy children and adults and in patients with chronic liver disesses. J Clin Microbiol 1999; 37 (6): 1829-3l.
40 - Nakano T, Park YM, Mizokami M, Choi JY, Orito E, Ohno T et al. TT virus infection among blood donors and patients with non-B, non-C liver diseases in Korea. J Hepatol 1999; 30 (3): 389-93.
41 - Kabayashi M, Chayama K, Arase Y, Tsubota A, Suzuki Y, Koida J eta al. Prevalence of TTV before and after blood transfusion in patients treated surgically for hepatocellular carcinoma. J Gastroenterol Hepatol 1999; 14 (3): 358-63.
42 - Utsunomiya S, Yoshika K, Takagi K, Wahita T. The prevalence of TTV infection and the route of TTV transmission in hemodialysis patients-compared with HCV infection. Nippon Rinsho 1999; 57 (6): 1417-20.
43 - Prati D, Lin YH, de Mattei C, Lui JK, Farma E, Ramaswamy L et al. A prospective study of TT Vius infection in transfusion-dependent patients with beta-thalassemia. Blood 1999; 93 (5): 1502-5.
44 - Hino K, Okuda M, Ishiko H, Okita K. Detection of TT virus in hemodialysed patients. Nippon Rinsho 1999; 57 (6): 1413-6.
45 - Ummemura T, Tanaka E, Kiyosawa K. TT virus infection in area of high-endemicity for hrpatitis C. Nippon Rinsho 1999; 57 (6): 1397-401.
46 - Davidson F, MacDonald D, Mokili JLK, Prescott LE, Graham S, Simmnonds P. Early acqusition of TT virus ( TTV) in area andemic for TTV infection. J Infect Dis 1999; 179 (5): 1070-6.
47 - Arakawa Y, Shioda A, Moriyama M. Incidence of TT virus infection in patients with non-A to G liver disease. Nippon Rinsho 1999 1999; 57 (6): 1290-4.
48 - Ikeda H, Takasu M, Inoue K, Okamoto H, Miyakawa Y, Mayumi M. Infection with an unenveloped DNA virus (TTV) in patients with acute or chronic liver disease of unknown etiology and in the patients positive for hepatitis C virus RNA. J Hepatol 1999; 30 (2): 205-12.
49 - Kanda T, Yokosuka O, Ikeuchi T, Seta T, Kawai S, Imazeki F, Saisho H, The role of TT virus infection in acute viral hepatitis. Hepatology 1999; 29 (6): 1905-8.
50 - Viazov S, Ross RS, Varenholz C, Lange R, Holtman M, Niel C, Roggendorf M. Lack of evidence for an association between TTV infection and severe liver disease. J Clin Microbiol 1998; 11 (3): 183-7.
51 - Schroter M, Feucht HH, Schafer P, Zollner B, Laufs R, Knodler B. TT virus viremia and liver transplantation. Blood 1998; l5 (92): 4877-8.
52 - Hohne M, Berg T, Muller AR, Schreier E. Detection of sequences of TT virus, a novel DNA virus, in Geram patients. J Gen Virol 1998; 79 (11): 2761-4.
53 - Tagger A, Donato F, Ribero ML, Binelli G, Gelatti U, Portera G et al. A case-control study on a novel DNA virus (TT virus) infection and hepatocelullar carcinoma. Hepatology 1999; 30 (1): 294-9.
56 - Itoh K, Hirakawa K, Okamoto H, Ukita M, Tanaka H, Sawada N et al. Infection by an unenveloped DNA virus aaociated with non A to G hepatitis in Japanese blood donors with or without elevated ALT levels. Transfusion 1999; 39 (5): 522-6.
57 - Zhou Y, Dong J, Zou Y. Molecular epidemiology of TT virus infection in some parts of China. Chung Hua Yu Fang I Hsueh Tsa Chih 1998; 32 (6): 352-5.
58 - Chayama K, Kobayashi M, Tsubota A, Kobayashi M, Arase Y, Suzuki Y et al. Suscebility of TT virus to interferon therapy. J Gen Virol 1999; 80 (3): 631-4.
59 - Takayama S, Miura T, Matsuo S, Taki M, Suguii S. Prevalence and persistence of a novel DNA TT virus (TTV) infection in Japanese haemophiliacs. Br J Haematol 1999; 104 (3): 626-9.
60 -Tsubota A. Clinical manifestations and histopathologic features of chronic liver disease with serum TT virus ( TTV) DNA positive alone measured by first generation primer sets. Nippon Rinsho 1999; 57 (6): 1345-9.