Alimentarni trakt i pankreas
ARCH GASTROENTEROHEPATOL 1999; 18 ( No 3 - 4 ):
Experts Comment
SEROUS CYSTIC TUMOURS OF THE PANCREAS
Serozni citsticni tumori pankreasa
Marjan Micev Milena Cosic - Micev
( accepted June 16¸ 1999 )
Department of Histopathology¸ Institute of Digestive Diseases¸Clinical Center of Serbia¸
Belgrade.
*************************************************************************
In the January 1999 issue of the Archives of Gastroenterohepatology¸ Atmatzidis et alpointed out the usefulness of frozen section biopsies in palliative management of the microcystic adenomas of the pancreas ( 1 ).We considered their report of interest to comment in relation to histogenesis andmalignant tumour potential linkage¸and diagnostic possibilities.
Unlike potentially malignant evolution of mucinous pancreatic cysts there is an evidence thatthe majority of serous cystic pancreatic tumours exibit a benign course( 2 - 4 ).Now there is the widespread management strategy whichavoidsunnecessary extensive operations. This increases the importance of the correct diagnosis.Preoperative diagnostic investigations areof paticular importance in diagnosing cytic nature of the pancreatic tumour and verifying its gross appearance ( 5 - 7 ).Ultrasonography¸ other imaging procedures¸ and angiography of the pancreatic cystic tumours are focused on division of thetwo types of cystic processes: the first¸ localised¸ low-density¸ hypervascularised microcystic¸ solid or mixed masses ; and the second¸ anechogenic¸ avascular¸ septated cystic changes of water density ( 8 - 11 ). The result wassimplified classifiication of cystic pancreatic neoplasms into two major types: microcystic¸ serous cystadenoma and macrocystic¸ mucinous cystic tumours which substantially differ in their long term prognosis and mortality.It became obviuous that such simplified macroscopicclassification was no longer tenable since variety of unusual gross tumours presentations and their variants were described. Reportsof microcystic serous adenoma with distinctive " honeycomb-like " or " sponge-like" appearances¸ macrocystic¸ oligocystic¸ unilocular¸ well mixed¸ and ill-demarcated or multicentric cystic neoplasms caused difficulties in interpretation ( 12 - 14 ).Very important is to recognise the solid gross variants of solid-cystic ( papillary-cystic ) adenomas because the great majority of such tumours are malignant ( 8¸15 - 17 ).It is also well known that microcystic and papillary neoplasms could be associated with mucin production; many of them malignant ( 18 - 20 ).
On the contrary to their macroscopic diversity¸ the histologic typing of neoplastic pancreatic cysts are less heterogenous. Their serous cystic proliferations appear to beclosely relatedwith benign biological behaviour.Histopathological verification of the benign nature of these tumoursis simply denoted as " cystadenomas " ( 21 - 23 ). But examples of serous cystadenocarcinoma and coexistence of serous cystic tumours and pancreatic carcinoma were already reported(11¸19¸24¸25 ). Long-term follow-up series of cystadenomas demonstrated their substantial rate of growth which neccessitated resection procedures. Few cases of very rapid tumour growth and freqeuent relapses were published ( 5¸6¸26¸27 ). There is an association of serous cystic pancreatic tumours with von Hippel-Lindau disease¸ Evans syndrome¸ sclerodermia and diabetes mellitus ( 7¸23¸28 - 30 ).Association with visceral cancers¸ including coexistent pancreatic carcinoma is of great interest because ofthe possibility of non-genotoxic pancreatic tumour promoters and p53 gene point mutations ( 11¸31 - 33 ). The tumour cell antigen reactivity and other ultrastructuralessays provide insufficient evidence of probable centroacinar r dual ductuloacinar origin of these neoplasms¸ nor an explanatation for striking difference in malignant potential of neoplastic cyst with mucinous ductal epithelial cell origin ( 15¸16¸25¸27¸34 ). There are few reports about diverse cell populations of pancreatic cystic tumours demonstrating the presence of myoepithelial cells¸ pericytes¸ and diffuse endocrine cells ( 12¸35¸36 ). It is not clear whether these cellular asortments have any influence on tumour biology.
Successful preoperative fine needle aspiration biopsy is either rarely achieved or provide insufficient tissue for histologic examination ( 37¸38 ). Intraoperative diagnosis ( frozen sectionbiopsies ) is therefore of particular importance. There are great difficulties in interpretation since it represents a pattern of histogenesis ather than differentiation¸ i.e. recognition of histological type of epithelial lining n favour of histological and cytological signs of malignancyis oftenly missing and requires definitive histopathology ( 1¸7¸18¸26¸27 ).This means the recognition of indicies of malignancy e.g. infiltrative margins¸ vascular invasion¸infiltration of urrounding structures¸ classical nuclear appearances and/or metastases.
In thelast 10 years we diagnosed 5 cases of benign pancreatic serous cystic tumours. The main clinical and pathological features are summerised in table 1. We could confirm tumour predominance in elderly woman¸ and its oligosymptomatic or asymptomatic clinical presentations. This explaines incidentaltumour findingasrather large intrapancreatic massess ( 3¸4¸7¸14¸34¸35¸39 - 42 ). Only two of our patients had tumourswith classical microcystic arrangement and central scarring.Figure 1¸2.The findings of multicentric and semi-solid cystic tumours¸ and ts rapid growth with postoperative recurence in one case rise the question hether tumour enucleation or palliative surgery is sufficient at all ? This is of particular importance in elderly patients because the extensive pancreatic sugery has
significant the inherent risk. Considering this it is very important to perform careful examination of the pancreas in order to determine whether coexisting carcinoma or satelitte nodules in multicentric tumours do exist¸ before concluding that patient ¸ s prognosis depends more on age related abnormalities.
*************************************************************************
REFERENCES
1.Atzamatzidis KS¸ Pavlidis TE¸ Lazaridis CN¸ Markris JG¸ Souparis AC¸ Papageorgiu A¸Papaziogas TV. Microcystic adenoma of thw pancreas: The usefulness of frozen section biopsy in palliatiove management. Arch Gastroenterohepatol 1999; 18: 5 - 7.
2.Borgne J. Cystic tumours of the pancreas. Br J Surg 1998; 85: 577 - 9.3.Martin I¸ Hammond P¸ Scott J¸ Rehead D¸ Carter D¸ Gargen O. Cystic tumours of the pancreas. Br J Surg 1998; 86: 1484 - 6.
4.Compagno J¸ Oertel J. Microcystic adenoma of the pancreas ( glycogen - rich cystadenomas ). A clinicopathologic study of 34 cases. Am J Clin Pathol 1978; 69: 289 - 98.
5.Gribbin C¸ Nosher JL¸ Miller R¸ Smilov P. Microcystic adnoma of the pancreas. N Engl J Med 1994; 91: 523 - 5.
6.Healy JC¸ Davies SE¸ Reznek RH. CT of microcystic ( serous ) pancreatic adenoma. J Comput Assist Tomograph 1994; 18: 146 - 8.
7.Le Borgne J. Pancreatic cystadenoma. Ann Chir 1989; 43: 451 - 7.
8.Itai Y¸ Ohhashi K¸ Furui S¸ et al. Microcystic adenoma of the pancreas: sepctrum of omputed tomographic finidngs. J Comput Assist Tomograph 1988; 12: 797 - 803.
9.Padovani B¸ Neuvet P¸ Chanalet S¸ et al. Microcystic adenoma of the pancreas: report on four cases and review of the literature. Gastrointest Radiol 1991; 16: 62 - 6.
10.Delcenserie R¸ Dupas JL¸ Joly JP¸ Dsecombes P¸ Mortier F¸ Capron JP. Microcystic
adenoma of the pancreas demonstrated by endoscopic retrograde cholangiopancreato- graphy. Gastrointest Endosc 1988; 34: 52 - 4.
11.Posniak HV¸ Olson MC¸ Demos TC. Coexistent adenocarcinoma and microcytic adenoma of the pancreas. Clin Imaging 1991; 15: 220 - 2.
12.Kim YI¸ Seo JW¸ Suh JS¸ Lee KU¸ Choe KJ. Microcystic adenomas of the pancreas-Report of three cases with two multicentric origin. Am J Clin Pathol 1990; 94: 150 - 6.
13.Lewandrowski K¸ Warshaw A¸ Compton C. Marocystic serous cystadenoma of the pancreas: a morphologic variant differing from microcystic adenoma. Hum Pathol 1992; 23: 871 - 5.
14.Egawa N¸ Maillet B¸ Schroder S¸ Mukai K¸ Kloppel G. Serous oligocystic and ill-demarcated adenoma of the pancreas: a variant of serous cystic adenoma. VirchowsArch 1994; 424: 13 . 7.
15.Perez-Ordonez B¸ Naseem A¸ Liberman PH¸ Klimstra DS. Solid serous adenoma of the pancreas. The solid variant of serous cystadenoma? Am J Surg Pathol 1996; 20: 1401 - 5.
16.Luchtrath H¸ Adams A. Solid cystic acinar cell tumor of the pancreas. Immunohistologic studies of histogenesis. Zentrabl Allg Pathol 1988; 134: 47 - 52.
17.Horie A¸ Haratke J¸ Jimi A¸ Matsumoto M¸ Ishii N¸ Tsutsumi Y. Pancreatoblastoma in Japan¸ with differential diagnosis from papillary cystic tumor ( ductuloscinar adenoma ) of the pancreas. Acta Pathol Jpn 1987; 37: 47 - 63.
18.Zahradka W¸ Ulbricht G. Cystic adenoma of the pancreas. Z Gesamte Inn Med 990; 45: 20 - 1.
9.Yoshida J¸ Ozaki H¸ Yamamoto J¸ et al. Adenocarcinoma and concomitant papillary adenoma in the pancreas. Jpn J Clin Oncol1991; 21: 453 - 6.
20.Obara T¸ Saitoh Y¸ Maguchi H¸ et al. Papillary adeoma of the pancreas with excessive mucin secretion. Pancreas 1992; 7: 114 - 7.
21.Heatly MK¸ McCrory DC¸ O ¸ HaraMD. Microcystic adenoma of the pancreas. Ulster Med J 1991; 60: 11 - 3.
22.Schmidt U¸ Donhuijsen K¸ Littmann K. Cystic adenoma of the pancreas. Verh Dtsch Ges Pathol 1987; 71: 317 - 21.
23.Labenz J¸ Borsch G¸ Rotzscher V¸ Breining H.Serous ( microcystic ) pancreatic adenoma. Fortschr Med 1980;107: 473 - 6.
24.George D¸ Murphy F¸ Michalski R¸ Ulmer B. Serous cystadenocarcinoma of the pancreas: a new entity? Am J Surg Pathol 1989; 13: 61 - 6.
25.Montag AG¸ Fossati N¸ Michelassi F. Pancreatic micocystic adenoma coexistent with pancreatic ductal carcinoma. A report of two cases.Am I Surg Pathol 1990; 14: 352 - 5.
26.Ben Othman M¸ Ben Romdhane K¸ Khattech R¸ Ammar A¸ Boughamni M¸ Rahal K.Microcystic adenoma of thepancreas. J Chir ( Paris ) 1995; 132: 206 - 8.
27.Radiolo C¸ Porta E¸ Berta V¸ Schiaffino E¸ Guarneri A. Microcystic serous cystadenoma of the pancreas. Enucleation or regulated pancreatic resection? Minerva Chir 1993; 48: 1269 - 74.
28.Torres-Barrera G¸ Fernandez-Del Castillo C¸ Reyes E¸ Robles-Diaz G¸ Campuzano M. Microcystic adenoma of the pancreas. Dig Dis Sci 1987; 32: 454 - 8.
29.Nyongo A¸ Huntrakoon M. Microcystic adenoma of the pancreas with myoepithelial cells. A hitherto undescribed morphologic feature. Am J Clin Pathol 1985; 84: 114 - 20.
30.Doll DC¸ List AF¸ Yarbro JW. Evans syndrome associated with microcystic adenoma of the pancreas. Cancer 1987; 59: 1366 - 8.
31.Pike J¸ Ehsani MT. Microcystic adenoma of the pancreas - an incidental finding. Austral Radiol 1989; 33: 404 - 5.
32.Wouterseon RA¸ van Garderen-Hoetmer A¸ Lamers CB¸ Scherer E. Early indicators of exocrine pancreas carcinogenesis produced by non-denotoxic agents. Mutat Res 1991; 248: 291 - 302.
33.Kaino M¸ Kondoh S¸ Okita S¸ et al. p35 mutations in two patients with intraductal papillary adenoma of the pancreas. Jpn J Cancer Res 1996; 87: 1195 - 8.
34.Alpert LC¸ Troung LD¸ Bossart MI¸ Spjut HJ. Microcystic adenoma ( serous cystadenoma ) of the pancreas. A study of 14 cases with immunohistochemical and electron-microscopic correlation. Am J Surg Pathol 1988; 12: 251 - 63.
35.Shorten SD¸ Hart WR¸ Petras RE. Microcystic adenomas ( serous cystadenomas ) of pancreas. A clinicopathologic investigation of eight cases with immunochistochemical and ultrastructural studies.Am J Surg Pathol 1986; 10: 365 - 72.
36.Kim YW¸ park YK¸ Lee S¸ et al. Panceaticandocrine tumor admixed with diffuse microcystic adenoma - a case report.J Korean Med Sci 1997; 12: 469 - 72.
37.HittmairA¸ Pernthaler H¸ Tozsch M; Schmid KW.Preoperative fine needle aspiration cytology of a microcystic adenoma of the pancreas. Acta Cytol 1991; 35: 546 - 8.
38.Nguyen GK¸ Vogelsang PJ. Microcystic adenoma of the pancreas. A report of two cases with fine needle aspiration cytology and differential diagnosis.Acta Cytol 1993; 37: 908 - 12.
39.Zogno C¸ Schiaffino E¸ Coci A¸ Schmid C¸ et al. Microcystic adenoma of the pancreas. Immunohistochemical and ultrastructural study of 7 cases. Pathologica 1994; 86: 623 - 9.
40.Spitale LS¸ de la Fuuente JL¸ Perez Gimenez PA¸ Saliba JA¸ Montenegro RB. Microcystic serous cystadenoma of pancreas. Clinicopathologic and surgical features.Acta Gastroenterol Latinoam 1997; 27: 39 - 42.
41.O ¸ Dell ML¸ Handler MS¸ Wetzel L. Indicantal detection of a microcystic adenoma of the pancreas. South Med J 1991; 84: 776 - 9.
42. Buck JL¸ Hayes WS. From the Archives of the AFIP. Microcystic adenoma of the pancreas. Radiographics 1990; 10: 313 - 22.
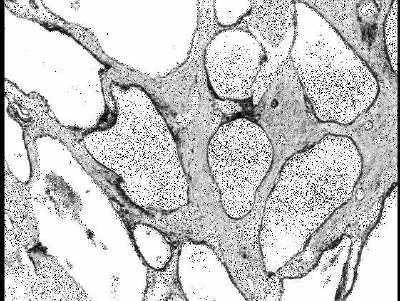
Figure 1. The distinceive feature of cystic tumoral organisation is acckmpanied with prominent fibrous septa ( H&E¸ 64x ).
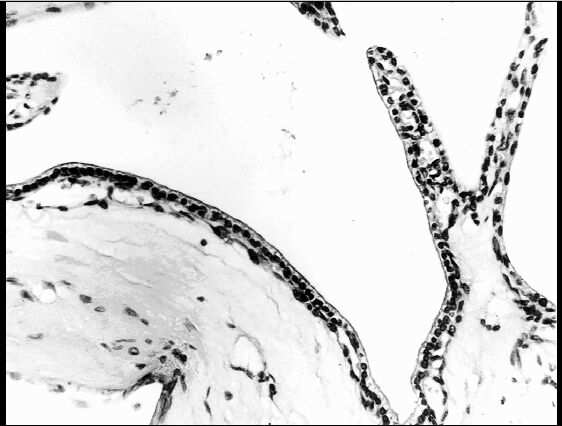
Figure 2. Slightly irregular thin-ealled cysts are lined with regular cuboidal single-layered epithelium ( H&E¸ 260x ).
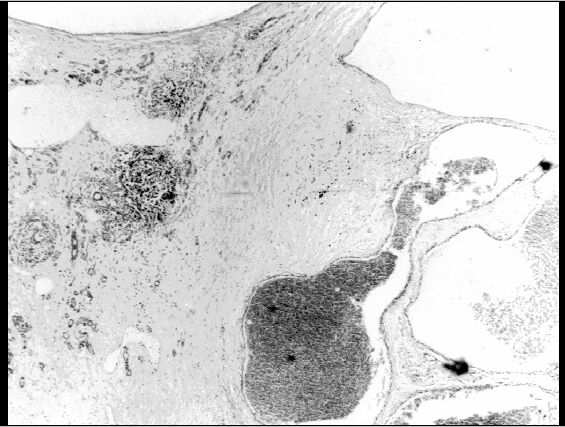
Figure 3. Oligo.macrocystic variant of serous cystic adenoma with foci of remnant pancreatic tissue in abundant fibrous stroma ( H&E¸ 64x
Table 1. Summary of the main clinico-pathological features of patients with benign
serous cystic pancreatic tumours in the Institute of Digestive Diseases¸ Clinical Center
of Serbia in a 10 year period ( 1989 - 1998 ).
| Case | Sex / Age | Clinical beckgraund | Tumor location | Size(cm) | Gross appearance | Surgery | Follow-up |
| 1. | F/59 | Rectal cancer (Incidental intraoperative finding) | Corpus and tail | 7.8 | Multicentric Macrocystic-microcystic | Distal pancreatectomy | Died after 3 years (Disseminated intestinal cancer) |
| 2. | F/66 | Abdominal pain¸ palpable mass Diabetes mellitus | Corpus | 8.5 | Macrocystic-solid | Distal pancreatectomy | Alive and well |
| 3. | F/74 | Retroperitoneal malignant fibrous histocytoma (Incidental intraoperative finding) | Tail | 2.6 | Microcystic | Tumor enucleation | Alive and well |
| 4. | M/62 | Epigastric pain Duodenal ulcer | Head | 9.2 | Multicentric Macrocystic | Tumor enucleation | Recurrence;rapid growth |
| 5. | F/70 | Jaundice¸ epigastric pain Diabetes mellitus | Head | 3.5 | Microcystic | Cephalic pancreato - duodenectomy | Died after 2 months (postoperative complications ) |