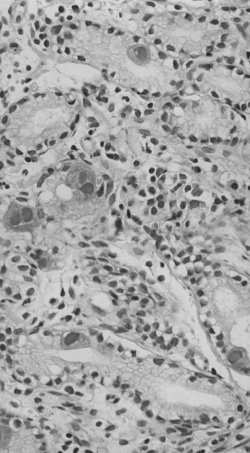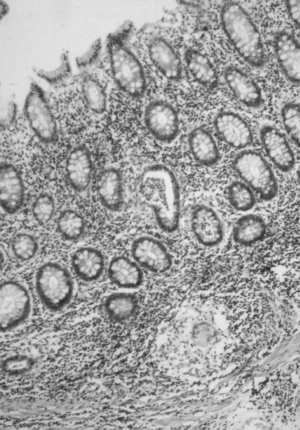
A 26-year old male was referred to our unit because of severe epigastric pain¸ nausea, and vomiting lasting for about couple of days. Since the age of 22, he was diagnosed as having ileo - caecal Crohn , s disease ( CD ). He experienced several relapses which were treated with metronidazole and prednisolone, but two years later surgery was performed. The histopathological report on resected ileo- caecal segment cofirmed the diagnosis of CD of penetretating type with multiple fistulous tracts. Postoperative course was uneventful for more than a year, when symptoms of coltitis reappered. Colonoscopic examination revealed segmental stenosis in sigmoid region with cobblestone appearance of the mucosa and biopsy showed focal chronic inflammation with granulomas. Figure 1. Since symptoms referred to gastric involvement of CD were present, gastroduodenoscopy was performed, revealing substantial mucosal changes as follow: distal stomach mucosal nodularity with multiple erosions, occasional small ulcerations, and thickened antral mucosal folds. In addition, x - ray examination demonstrated antral luminal narrowing, rigidity, and intramural thickening. The histology of mucosal biopsies showed an obvious inflammation of non - homogenous distribution, moderate increase of inflammatory cells in the lamina propria, and erosive defects. However, there were prominent viral inclusions, both nuclear and cytoplasmatic in foveolar epithelium and mucous neck cells, and rarely in endothelial and mesenchymal stromal cells suggesting diagnosis of cytomegalovirus ( CMV ) gastritis. Figure 2. There was no evidence of underlying risk factors or medical conditions predisposing to CMV infection such as immunosupressive administration, transplantation, HIV positivity etc.
Comment An unusual presentation of CD and CMV infection recapitulates contraversies on etiopathogenesis of inflammatory bowel disease ( IBD ) ( 1 ). There are no pertinent facts of causative role of microbial agents, but many candidates appear to be involved in the pathogenesis of IBD. Besides experimental and clinical data supporting potential role of Mycobacterium paratuberculosis and Listeria monocytogenes, the " granulomatous vasculitis " concept of CD became more attractive after measles virus, its mRNA, and paramyxovirus - like structures visualisation within endothelium and granulomas ( 2 - 4 ). This may suggest possibility of persistent viral infection in the etiopathogenesis of IBD. Howevere, this phenomenon was demonstrated only in subset of patients with CD. Further on, there was no singificance in antibody titers for measles virus , CMV, adenovirus, and herpes simplex virus in patients with CD and controls ( 5 ).
All in all, there is no strong evidence for etiological role of virusis in IBD, including measles virus and CMV ( 13 - 15 ). Reports of gastrointestinal CMV infections in patients with IBD indicating viral infection as an aggraviating factor only are few. On the contrary, it may be assumed that CMV gastrointestinal infection causing vasculitis of small mucosal vessels may be an introductory penomenon leading to further pathogenetic changes ( 6 - 12 ). Ananalogy could be made with CMV and some other stomach infections, including Helicobacter pylori and possible gastric involvement of CD ( 11,12 ). In addition, both conditions ( CMV and Crohn's gastritis ) might have the same presentation with focal transmural inflammation, deep mucosal ulcerations, and possible penetration or stricturing without distinctive features such as viral inclusions and granulomas ( 16 - 21 ). ********************************************************************************
REFERENCES:
1. Hodgson HJF. Pathogenesis of Crohn's disease. Baill Clin Gastroenterol 1998; 12: 1 - 17.
2.Wakefield AJ, Sim R, Akbar AN, Pounder RE, Dhillon AP. In situ immune responses in Crohn's disease: a comparisson with acute and persistent measles virus infection. J Med Virol 1997; 51: 90 - 100.
3.Daszak P, PurcellM, Lewin J, Dhillon AP, Pounder RE, Wakefield AJ. Detection and comparative analysis of persistent measles virus infection in Crohn's disease by immunogold electron microscopy. J Clin Pathol 1997; 50: 299 - 304.
4.Thompson NP, Montgomery SM, Pounder RE, Wakefield AJ. Measles vaccination: a risk factor in inflammatory bowel disease? Lancet 1995; 345: 1071 - 3.
5.Fisher NC, Yee L, Nightingale P, McEwan R, Gibson JA. Measles virus serology in Crohn's disease. Gut 1997; 41: 66 - 9.
6.Christ AD, Sieber CC, Cathomas G, Gyr K. Concomitant active Crohn's disease and acquired ommunodeficiency syndrome. Scand J Gastroenterol 1996; 31: 733 - 5.
7.Sebastian - Planas M, Merino - Barrio A, Avilla - Hernandez J, et al. Cytomegalovirus infection of the colon in ulcerative colitis: a pediatric case. J Ped Gastroenterol Nutr 1996; 23: 186 - 90.
8.Page MJ, Dreese JC, Poritz LS, Koltun WA. Cytomegaloenteritis: a highly lethal condition requiring early detection and intervention. Dis Colon Rectum 1998; 41: 619 - 23.
9.Roskel DE, Hyde GM, Campbell AP, Jewell DP, Gray W. HIV associated cytomegalovirus colitis as a mimick of inflammatory bowel disease. Gut 1995; 37: 148 - 50. 10.D , Haens GR, Suenaret P, Westhovens R, Rutgers P. Severe knee pain as single symptom of CMV infection in acute ulcerative colitis treated with cyclosporin. Inflamm Bowel Dis 1998; 4: 27 - 8.
11.Van Thiel DH, Gavaler JS, Schade RR, Chien MC, Starzl TE. Cytomegalovirus infection and gastric empying. Transplantation 1992; 54: 70 - 3. 12.Aquel NM, Tanner P, Drury A, Francis ND, Henry K. Cytomegalovirus gastritis with perforation and gastrocolic fistula formation. Histopathol 1991; 18: 165 - 8.
13.Haga Y, Funakoshi O, Kuroe K, et al. Absence of measles virus genomic sequence in intestinal tissues from Crohn , s disease by nested polymerase chain reaction. Gut 1996; 38: 21 - 5.
14.Walmseley RS, Anthony A, Sim R, Ponder RE, Wakefield AJ. Absence of Escherichia coli, Listeria monocytogenes and Klebsiella pneumoniae antigens within inflammatory bowel disease tissue. J Clin Pathol 1998; 51: 657 - 61.
15.Chiba M, Fukushima T, Horie Y, Iizuka M, Masamune O. No Mycobacterium paratuberculosis detected in intestinal tissue, including Payer , s patches and lymph follicles of Crohn , s disease. J Gastroenterol 1998; 33: 482 - 7.
16.Halme L, Karkkainen P, Rautelin H, Kosunen TU, Sipponen P. High frequency of Helicobacter negative gastritis in patients with Crohn's disease. Gut 1996; 38: 379 - 83.
17.Meining A, Bayerdorfer E, Bastlein E, et al. Focal inflammatory infiltrations in gastric biopsy specimens are suggestive of Crohn's disease. Scand J Gastroenterol 1997; 32: 813 - 8.
18.Oberhuber G, Hirsch M, Stolte M. High incidence of upper gastrointestinal tract involvement in Crohn's disease. Virchows Arch 1998; 432: 49 - 52. 19.Wagtmans MJ, Verspaget HW, Lamers CBHW, von Hogezand RA. Clinical aspect of Crohn's disease of the upper gastrointestinal tract: A comparison with distal Crohn's disease. Am J Gastroenterol 1997; 92: 1467 - 71.
20. Wagtmans MJ, van Hogezand RA, Griffioen G, Verspaget HW, Lamers CB. Crohn , s disease of the upper gastrointestinal tract. Neth J Med 1997; 5o: S2 - 7.
21.Oberhuber G, Puspok A, Oesterreicher C, et al. Focally enhanced gastritis: a frequent type of gastritis in patients with Crohn's disease. Gastronterology 1997; 112: 698 - 706.