Liver and biliary tract
Jetra i bilijarni trakt
ARCH GASTROENTEROHEPATOL 2001; 20 ( No 1 – 2 ):
THE SIGNIFICANCE OF SHUNT SURGERY IN TREATMENT OF PORTAL HYPERTENSION
Značaj šant hirurgije u lečenju portne hipertenzije
( accepted March 31st, 2001 )
Rada Ješić, 1Bozina Radević, 1Dragan Sagić, Dragan Tomić, Miodrag Krstić, Tamara Aleksić, Tanja Cvejić, Vladislava Bulat, Radmila Šarenac, Djordje Ćulafić, Mirko Bulajić.
Institute of Digestive Diseases, Clinic for Gastroenterology and Hepatology, Clinical Center of Serbia, Belgrade, 1Institute for Cardiovascular Diseases Dedinje, Belgrade.
Address correspondence to: Professor Dr Rada Ješić
Clinic for Gastroenterology and
Hepatology,
Institute of Digestive Diseases,
Clinical Center of Serbia,
Koste Todorovića 6 St.,
YU-11000 Belgrade, Serbia,
Yugoslavia.
Tel + 381 11 361 777/ Ext. 3733
************************* *************************
Surgery of portal hypertension Gastroenterološka sekcija SLD,
01703, 2001
ABSTRACT
From October 1995 until December 1999, 39 consecutive patients ( age range: 17 – 64 years ) with portal hypertension of different aetiology underwent shunt surgery. Patients were divided into 3 groups: the first group, ( 19, 48.7% ) cases with alcoholic cirrhosis; the second group, ( 14, 35.8% ) patients with non-alcoholic liver disease; the third group, ( 6, 15.3% ) cases with other aetiologies. Twenty-six patients were of Child-Pugh class B, 13 cases Child-Pugh class C. Type of the shunt was related on patient’s hemodynamic characteristics, clinical condition, and aetiology of portal hypertension. Distal spleno-renal shunt was made in 20 patients. In six patients this was combined with partial splenic resection. Fifteen cases underwent mesocaval shunt with H-graft, while in 4 patients coronaro-caval shunt was made.
Postoperative follow-up studies demonstrated stable liver function tests in 36 cases. Variceal size was greatly reduced in 27 patients. No variceal bleeding occurred during the immediate postoperative period. Haematologic indices of hypersplenism were reversed in 18 cases. Ascites did not recur in 27 patients. In 4 cases shunts became thrombosed. In the very first 2 cases this occurred during immediate postoperative period, in another 2 after couple of years. Acute postoperative encephalopathy was recorded in 3 patients, while chronic in 4 cases. Hepatic perfusion index was slightly decreased in 4 patients. Thirty-four patients survived from 2.5 to 4.5 years in average.
Key words: portal hypertension, variceal haemorrhage, shunt surgery.
SAZETAK
Od Oktobra 1995 godine do Decembra 1999 godine, 39 bolesnika ( zivotna dob: 17 – 64 godine )sa portnom hipertenzijom je bilo podvrgnuto šant operacijama. Pacijenti su bili podeljeni u tri grupe. U prvoj ( 19, 48.7% ) su bili oni sa alkoholnom cirozom, u drugoj ( 14, 35.8% ) bolesnici sa ne-alkoholnim bolestima jetre, u trećoj ( 6, 15.3% ) slučajevi sa oboljenjima jetre najrazličitije etiologije. Prema klasifikaciji Child-Pugh, 26 bolesnika je bilo u klasi B, 13 u klasi C. U svakog pacijenta izbor šant operacije je zavisio od utvrdjenih hemodinamskih karakteristika, kliničkog stanja, i etiologije portne hipertenzije. Distalni spleno-renalni šant je načinjen u 20 bolesnika ( u 6 kombinovan sa parcijalnom resekcijom slezine ), mezo-kavalni sa H-graftom u 15, a u 4 koronaro-kavalni šant.
Postoperativno testovi jetrinih funkcija se nisu izmenili u 36 operisanih. Veličina variksa se značajno smanjila u 27. U neposrednom postoperativnom periodu ni u jednog bolesnika nije došlo do ponavljanja variksnih hemoragija. Posle operacije u 18 pacijenata je došlo do normalizacije hematoloških pokazatelja hipersplenizma. Ascent izliv se u potpunosti povukao u 13 bolesnika. Tromboza šanta se dogodila u 4 operisanih i to u 2 u neposrednom postoperativnom periodu, a u 2 posle 2 godine. Akutna postoperativna encefalopatija je registrovana u 3, a hronična u 4 bolesnika. Hepatični perfuzioni indeks je bio blago snizen u 4 operisanih. Prosečno prezivljavanje je u 34 operisanih bilo izmedju 2.5 - 4.5 godina.
Ključne reči: portna hipertenzija, varicealno krvarenje, šant.
INTRODUCTION
Portal hypertension is a clinical syndrome characterized by an elevation of portal blood pressure above 10 mmHg. Portal hypertension is general result of a combination of increased portal blood flow and/or increased portal resistance. Signs and symptoms are primarily result of decompression of this elevated portal blood pressure through porto-systemic collaterals. Clinical consequences of the latter are varices: gastro-eosophageal, ano-rectal, retroperitoneal, and others. Patients with cirrhosis who develop large oesophageal varices have a 35% risk of variceal haemorrhage and 30-50% mortality rate associated with the bleeding episode ( 1 ).
PATIENTS AND METHODS
From October 1995 to December 1999, 39 consecutive patients with portal hypertension, variceal bleeding, ascites, and hypersplenismus who were admitted at the Clinic for Gastroenterology and Hepatology, Clinical Center of Serbia underwent shunt surgery at the Institute for Cardiovascular Diseases Dedinje. Preoperative assessment of lieno-portal system and liver function tests were made on the basis of ultrasound examination combined with Doppler technique, upper GI endoscopy, lieno-portal and mesenteric angiography, blood biochemistry, neurological profile assessment, and liver histology.
RESULTS
Thirty – nine patients enrolled this study. There were 28 males and 11 females. Age range was 17 to 64 years, average 43.5. The patients were divided into 3 groups: group 1, 19 ( 48.7% ) patients with alcoholic cirrhosis; group 2, 14 ( 35.8% ) with non-alcoholic liver disease; group 3, 6 ( 15.3% ) with other aetiologies. Twenty-six were of Child-Pugh class B, while 13 of Child-Pugh class C. Thirty-two patients bled from oesophageal and gastric varices. Seventeen had oesophageal varices grade III-IV, 9 varices grade II-III, 6 gastric varices, 10 had endoscopic evidence of portal gastropathy. Ascites was found in 13 cases, while 19 showed haematological indices of severe hypersplenismus. Indirect lieno-portography and mesenteric angiography performed at the Institute for Cardiovascular Diseases Dedinje revealed portal vein obstruction in 13 patients, portal and splenic vein occlusion in 4, and porto-lieno-mesenteric thrombosis in 3 cases. FIGURE 2. This was confirmed by lieno-portal US examination with Doppler technique in every case. FIGURE 1. The standard protocol treatment for patients with bleeding oesophageal varices consisted of intravenous infusion of somatostatin or vasopressin, endoscopic injection sclerotherapy, and Sengstaken-Blackmore tube tamponade in 9 cases.
Distal spleno-renal shunt was made in 20 patients. This operation was combined with partial splenic resection in 6 cases due to enormous splenic size and severe hypersplenismus. Meso-caval shunt with 8 mm H-graft was performed in 15 patients while 4 patients underwent coronaro-caval anastomosis. After operation liver function tests remained stable in 36 cases. Galactose elimination capacity test was made in 10 patients, and demonstrated values exceeding 300mg/min in all subjects.
After shunt surgery variceal size was greatly diminished in 27 patients. There was no repeated variceal haemorrhage postoperatively. In 18 cases haematological indices of hypersplenismus were reversed after operation. Clinically ascites disappeared in 13 cases, while small quantity of abdominal fluid persisted in 7 patients what was easy to control with small doses of diuretics.
Shunt occlusion occurred in 4 patients. In the first two cases this was recorded immediately after operation. In the remainder, after couple of years. An increased in splenic size, ongoing haematological abnormalities, color Doppler and angiographic examinations were important in diagnosing this complication.
Postoperative acute encephalopathy complicated shunt surgery in 3 patients. This patients checks- up demonstrated ensuing chronic moderate encephalopathy. From the beginning chronic mild encephalopathy was recorded in the another 4 cases. Hepatic perfusion index (total blood flow / portal blood flow ratio ) was > 30% of normal values ( normal values 56+ 24% ) in 25 tested patients postoperatively. The average survival of 34 patients, which were followed on the regular bases, was 4.5 years ( range: 2.5 – 4.5 years ).
DISCUSSION
Historically the primary management of portal hypertension has been changing encompassing porto-systemic shunting, pharmacological treatment, endoscopic sclerotherapy/ligation, devascularisation methods, and liver transplantation ( 7 ). The surgical wisdom of shunt operations was to permanently decompress the portal system below the values, which generates significant porto-systemic collateral blood flow and variceal haemorrhage without interrupting hepatic portal perfusion ( 6 ). It is therefore very important to evaluate in every adult case with portal hypertension pre-existing liver disease and to determine its aetiology. This has to be followed by portal venous system assessment including collaterals, measurement of portal pressure, and hepatic metabolic capacity testing which reflects hepatocytes functional mass. Hepatic functional reserve ( Child , s score ), functional tests ( MEGX and galactose-elimination ), and portal perfusion assessment are important predictors in planing whether the individual patients has to be subjected to shunt operation, endoscopic variceal obliteration, devascularization procedures, or liver transplantation ( 1,8,9,10 ).
There is an evidence that liver function tests and portal perfusion rate are scoring better in patients with alcoholic cirrhosis and bleeding varices who underwent sclerotherapy/ligation rather than shunt surgery. Their survival rate is similar to those with non-alcoholic liver cirrhosis and portal hypertension treated with distal spleno-renal shunt ( DSRS ) ( 11 ). On the contrary there is evidence that in patients with alcoholic cirrhosis DSRS with spleno-pancreatic disconnection enhances portal perfusion and survival rate compared with standard DSRS. In non-alcoholic cirrhosis there is no evidence that DSRS combined with spleno-pancreatic disconnection is more beneficial than standard DSRS ( 12 ). In patients with stabile liver disease in which galactose-elimination test is equal or greater then 300 mg/min and the liver volume exceeds 75% of the normal values selective shunt is preferable. This was confirmed with our experience with patients with alcoholic cirrhosis of Child-Pugh class B and C, and stable liver disease that underwent DSRS.
There are some groups which advocate DSRS in compensated Child A and B cirrhosis, while C and decompensated Child B cirrhosis have to be managed by portocaval, mesocaval shunt or oesophageal transection with splenectomy ( 2, 13 ). Paquet et al reported that DSRS is preferable when portal perfusion index ( PPI ) is > 30% of normal values, while small diameter meso-caval interposition shunt when PPI is between 10-30% of normal values ( 14 ). This emphasizes the importance of proper selection of candidates for particular form of shunt, which may significantly reduce the risk of postoperative encephalopathy ( 15,16,17 ). Spina et al defined preoperative independent predictive prognostic risk factors for the development of encephalopathy: age of the patient, serum albumin level, and the existing hepatofugal flow. In our group of patients hepatic encephalopathy was recorded after shunt surgery. This was managed by protein reduction to 60 gr/day and Lactitol administration ( 25-50 mg/day ).
An increase of platelet count is important screening test for DSRS patency ( 18 ). Trombocytopenia due to hypersplenismus is primarily caused by platelet sequestration by enlarged spleen which may keep up to 90% of trombocytes. In significant number of patients leukopenia and anemia are present as well. In these cases DSRS combined with partial splenic resection may reverse all haematologic abnormalities. In our series of operated patients 18 demonstrated haematoloical restitution.
In conclusion our results indicate in properly selected patients beside other treatment modalities shunt surgery has definite role in the treatment of portal hypertension. When pharmacological measures, endocopic variceal obliteration procedures, and shunt surgery fail, persisting portal hypertension with variceal haemorrhage in an indication for liver transplantation ( 5 ).
REFERENCES:
1.Rikkers LF, Jin G. Emergency shunt. Role in the present management of variceal bleeding. Arch Surg 1995; 118: 472-7.
2.Collini FJ, Brener B. Portal hypertension. Surg Ginecol Obstet 1990: 170: 177-92.
3.Rikkers L. Bleeding esophageal varices. Surg Clin North Am 1987; 67: 475-88.
4.Kanaya S, Katoh H. Long-term evaluation of distal spleno-renal shunt with spleno-pancreatic and gastric disconnection. Surgery 1995; 118: 28-35.
5.Radevic B. Decompresivni sant I resekcija slezine.U: Radevic B, Perisic VN, Sagic D. ( eds ). Porta hipertenzija. Beograd:Zavet, 1999; 233-5.
6.Rikkers LF, Jin G. Variceal haemorrhage: surgical therapy. Gastroenterol Clin North Am 1993; 22: 821-42.
7.Rhee P, Sarfeh IJ.Portal hypertension. Curr Opin Gen Surg 1993; 22: 249-56.
8.Albuquuerque LA, Olivera A. Surgical treatment of portal hypertension in patients with liver cirrhosis. Arch Gastroenterol 1988; 25: 218-23.
9.Rikkers LF. Definitive therapy for variceal bleeding. A personal view. Am J Surg 1990; 160: 80-5.
10.Orloff MJ, Orloff MS, Rambotti M. Is portal-systemic shunt worthwile in Child class C cirrhosis? Long-term results of emergency shunt in 94 patients with bleeding varices. Ann Surg 1992; 16: 256-66.
11.Grece ND, Conn HO, Resnick RH. Distal spleno-renal vs portal-systemic shunt after hemorrhage from varices: a randomized controlled trial. Hepatology 1988; 8: 1475-81.
12.Gusberg RJ. Selective shunt in selected older cirrhosis patients with variceal heemorrhage. Am J Surg 1993; 166: 274-8.
13.Lacy AM, Navasa M, Gilabert R. Long-term effects of distal spleno-renal shunt on hepatic hemodunamics and liver function in patients with cirrhosis; importance of reversal of portal blood flow. Hepatology 1992; 15: 616-22.
14.Paquet KJ, Mercado MA, Klingele H. Investigation of the portal perfusion index after low diameter meso-caval interposition and distal spleno-renal shunt – a prospective study. Surg Endosco 1991; 5: 204-8.
15.Spina GP, Santambrogio R. factors predicting chronic hepatic encephalopathy after distal spleno-renal shunt: a multivariate analysis of chronic and hemodynamic variables. Surgery 1993; 114: 519-26.
16.Hashimoto N. Ashida H, Kotoura Y. Analysis of hepatic encephalopathy after distal spleno-renal shunt. Hepatogastroenterology 1993; 40: 360: 4.
17.Riggio O, Balducci G, Ariosto F. Lactitol in prevention of recurerent episodes of hepatic encephalopathy in cirrhotic patients with portal-systemic shunt. Dig Dis Sci 1989; 34: 823-7.
18.Lodge JP, Mauor AI, Giles GR. Dos the Warren shunt correct hypersplenismus. HPB Surg 1990; 2: 41-7.
19.Ashida H, Takagi K, Nishioka A. Hemodynamic changes in splenic blood flow during and after distal spleno-renal shunt. Am J Gastroenterol 1990; 85: 1609-13.
20.Moreno E, Rico P, Seone J. Long-term results after shunt operation for portal hypertension. Hepatogastroenetrology 1991; 38: 1-3.

Figure 1. Percutaneous lieno-portography after distal spleno-renal shunt.

Figure 2. Distal splenic vein thrombosis. Note complete collateral circulation through inferior mesenteric vein ( VMI ).
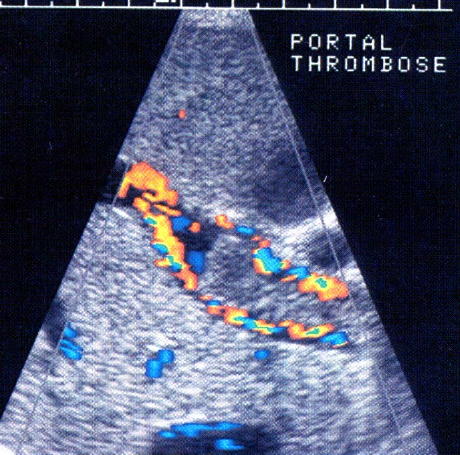
Figure 3. Color Doppler portography: portal vein dilatation in portal hypertension