We read it for you
Journal: Histopathology 2000; 36: 41 - 46
Title: Diversion colitis in children: an iatrogenic appendix vermiformis?
Diverzioni kolitis u dece: jatrogeni apendiks vermiformis?
Authors: *Vujanic GM, Dojcinov SD.
Institution: Department of Pathology, University of Wales, College of Medicine, Cardiff, UK.
ABSTRACT
Aims: Diversion colitis ( DC ) is a localised, relatively benign, iatrogenic condition, which occurs in almost 100% of, diverted colonic segments in patients who undergo ileostomy/colostomy for various reasons. The aim of this study was to establish histological features of DC in children.
Methods and results: twenty-three cases of DC following colostomy for Hirschprung , s disease in young children were analysed. The distinguishing features included prominent follicular lymphoid hyperplasia ( 100% ), chronic mucosal inflammation ( 100% ), accompanied by variable degree of acute inflammation ( 78% ) and Paneth cells metaplasia ( 26% ). Less frequent histological findings were as follow: mild goblet depletion ( 22% ), foci of cryptitis ( 13% ), crypt abscesses ( 13% ) and mild architectural distortion ( 22% ). A previously unrecognised feature was the presence of mucosal aggregates of eosinophils, found in 43% of cases. A striking similarity between the normal appearance of the vermiform appendix and pathological features in DC was noted and the possible relationship between the two is discussed.
Conclusion: Histological features of DC in children are very similar to those described in adults. They should help to distinguish it from ulcerative colitis and Hirschprung , s associated enterocolitis in order to prevent inappropriate therapy and follow-up. There are many similarities between DC and the normal appendix vermiformis.
EDITOR'S DIGEST
Diversion colitis ( DC is a process that develops in the by-passed segment of the large bowel after surgical diversion of the faecal stream. In adults reasons for diversions are diverticular disease, carcinoma, trauma, perianal fistulas, Crohn , s colitis and neurological faecal incontinence. In paediatric cases it has been reported in colon defunctionalised by proximal colostomy due to Hirschprung , s disease or colonic pseudoobstruction.
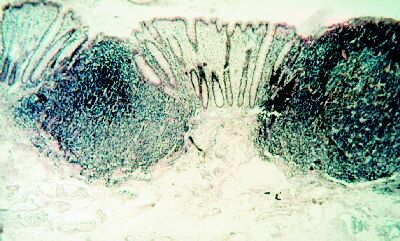
In adults morphological changes in DC depends of the underlying disease of the prediverted mucosa. Therefore, the spectrum of these changes is very wide. In paediatric cases diversion is usually done due to Hirschprung , s disease. Children demonstrate constant histological features: lymphoid follicular hyperplasia and diffuse mild-to-moderate chronic inflammation limited to mucosa. Figure 1.
Histological review of the study cases highlighted a striking morphological similarity between the histology of DC and normal appendix. Because the appendix is part of the large bowel and in continuity with the colon one would expect that they had many features in common. Interestingly, there are number of comparative differences between colon and appendix. First of all, prevailing bacterial flora in both sites is different: in75% of healthy appendices the flora is predominantly aerobic whilst it is predominantly anaerobic in the normal colon, but then reverse occurs in DC. The net flow of the luminal content in the normal, healthy appendix is exclusively outward (towards caecum ), this mimicking DC. Finally, the pattern of immunoglobulin expression in the appendix is different from that of the colon but there are no studies so far dealing with this aspect of DC. All these features show that these two organs behave differently in normal circumstances.
It is now established that DC is not a progressive disease, but rather an adaptation to the newly created microbial environment. This environment is similar to the existing in the normal appendix and in author , s view results also in morphological similarities.
DC was initially thought to arise as result of deficiency of mucosotrophic substances present in faeces, namely short chain fatty acids ( SCFAs ). One of them, faecal butiric acid is trophic to colonic mucosa. Treatment of DC with SFCAs has shown inconsistent results varying from complete clinical and histological remission to no histological and endoscopic improvement. It has been suggested that butyrate may influence constitutional and cytokine-mediated expression of molecules with immune functions and that its deficiency might influence a mucosal immune response. It remains to be determined whether or not both the pathological features of DC and the specific histological features of the appendiceal mucosa are the result of deprivation of mucosa from SFCAs.
* Dr GM Vujanic, Consultant Senior Lecturer in Paediatric Pathology University of Wales College of Medicine is member of the International Advisory Board of the Archives of Gasteroenterohepatology.