

Figure 1a, 1b. Barium study of the upper gastrointestinal tract demonstrating a round pancreatic rest in the antrum pyloricum.
ECTOPIC PANCREAS IN THE GASTRIC WALL
Ektopicni pankreas u zidu zeludca
( accepted September 10th¸ 1999 )
Tomica Milosavljevic, 1Vojislav Periic, 2Dejan Opric, Marjan Micev, Viktorija Korneti, Nada Kovacevic, Dragan Popovic, 3Radoslav Miloevic
Institute of Digestive Diseases, Clinical Center of Serbia, Belgrade
1 University Children's Hospital, Belgrade¸ 2 Institute of Pathology of Belgrade School of Medicine, 3cacak General Hospital, cacak
Address correspondence to:
Tomica Milosavljevic, MD, PhD.
Associate Professor of Medicine
Institute of Digestive Diseases, Clinical Center of Serbia
11000 Belgrade, 6 Koste Todorovica
Fax ( 381 11 ) 361 54 32
E-mail: [email protected]
Ectopic pancreas Milosavljevic T. et al.
ABSTRACT
Ectopic pancreas¸ aberrant or heterotopic pancreatic tissue, which is oftenly referred as pancreatic rest can be, found anywhere along the foregut and proximal midgut. This usually causes no symptoms. At autopsy, the frequency of ectopic pancreas is between 1 - 2% ( range 0.55% to 13% ); in surgical series 1 per 500 of upper abdominal laparotomies.
We report 4 patients with endoscopically diagnosed aberrant pancreas. In all cases the pancreatic rest was in antral and prepyloric, and diagnosed incidentally except case 1 which reatedly bled. In other 3 patients clinical symptoms were nonspecific. In all cases histological analyses were successful after standard endoscopic biopsies. Because of repeated episodes of upper GI bleeding patient 1 was operated eventually. Others were regularly followed endoscopically and there were no complications.
Key words: stomach¸ ectopic pancreas¸ endoscopy¸ surgery.
SAZETAK
Ektopicni ili aberantni pankreas¸ odnosno pankreasna heterotopija se uobicajeno dijagnostikuje u gornjim ili srednjim delovima alimentarnog trakta. On najcece ne prouzrokuje specificne simptome i znake. Ucestalost iznosi izmedju 1 - 2% ( varijacije izmedju 0.55% do 13% ); u hirurkim serijama u 1 od 500 operativnih zahvata u gornjim segmentima trbuha.U radu prikazjemo 4 pacijenta sa endoskopski dijagnosticiranim aberantnim pankreasom u zeludcu. Kod svih lokalizacija je bila u prepiloricnom delu i utvrdjena je slucajno prilikom traganja za organskim promenama u gornjim delovima alimentarnog trakta. Klinicki simptomi su bili nespicifini osim u pacijenta 1 koji je imao ponavljano proksimalno gastrointestinalno krvarenje i koji je lecen hirurki. U svim slucajevima histoloka dijagnoza je postavljena posle endoskopskih biopsija. Svi ostali bolesnici su endoskopski praceni i ni u jednog nije otkrivena ni jedna od mogucih komplikacija.
Kljucne reci: zeludac¸ ektopicni pankreas¸ endoskopija¸ hirurgija.
INTRODUCTION
Pancreatic ectopy (synonymous heterotopic¸ accessory¸ or aberrant pancreas etc.) is defined as the presence of pancreatic tissue lacking anatomic and vascular continuity with the main body of the gland (1¸2¸3 ). It can be found anywhere along the foregut and proximal midgut and usually causes no symptoms (1¸2¸3 ). About 75% of all pancreatic rests are located in the stomach, duodenum, or jejunum ( 1 ). However they have also been found in the ileum. Mockels diverticulum¸ the gallbladder, the common bile duct, the splenic hilum, the umbilicus, the lung, and in perigastric and periduodenal tissue ( 2 ). In autopsy series the frequency of ectopic pancreas is between 1 - 2% ( range: 0.55 - 13% ). The rate of recognition at the time of laparotomy is 0.2%. In endoscopic practice ectopic pancreas is oftenly diagnosed and sometimes imposes differential diagnostic problems ( 1,2,3 ).
Here we present our experience with the cases of ectopic pancreas located in the gastric wall.
MATERIAL AND METODS
We retrospectively analysed patient ¸ s records during last past 5 years in Endoscopy Department of the Institute of Digestive Diseases, with emphasis on patients with ectopic pancreas in the stomach proved by histological analyses.
RESULTS
We report 4 patients with with endoscopic diagnosis of aberrant pancreas. In all cases localisation of the pancreatic rest was in antral, prepyloric part of the stomach. Table 1. Ectopic pancreas was found incidentally during routine upper GI endoscopies. In one case the indication for oesophagogastrodudenoscopy was repeated upper GI haemorrhage. This patient was treated surgically. In other 3 cases clinical symptoms were nonspecific, and therefore they were followed endoscopically, once per year. Up to now complications were not recorded. In all cases histological analyses were successful after standard endoscopic biopsies.
DISCUSSION
The pancreas develops from two primordial diverticula of the duodenum and becomes apparent at 4th week of gestation ( 3 ). After axial rortation of the gut¸ the mesoduodenum fuses with the posterior peritoneum and forms the most
part of the duodenum. Fusion of the two pancreatic buds occurs simultaneously.
During pancreatic organogenesis, a number of embryological "mistakes" can happen. Pancreatic developmental errors can be classified as failures of migration or fusion and ductal anomalies. Table 2.
A fourth miscellaneous group of anomalies includes ectopic pancreas. It is unlikely that a single embiologic mechanism can account for this anomaly. Multiple ventral pancreatic buds development their failure to atrophy and subsequent growth, and sequestration may rise ectopic pancreas. Horgan and Whartin suggested that adhesion of portions of the dorsal and ventral pancreatic primordia to the neighboring structures during elongation and rotation of the gut may rise ectopic pancreas. Alternatively budding of pancreatic tissue from the embryonic anlagen with attachment to the gut wall and subsequent separation may causes ectopic pancreas as well. It has been suggested that multipotential cells from the primitive gut, capable of specialised differentiation may form pancreatic rests ( 3 ). Because of the close development of the embryonic pancreatic primordial buds to the foregut¸ it not surprising that 70 - 90% of pancreatic ectopia occurs in the upper GI system. Most ectopic pancreas in the upper GI tract are found in the gastic antrum: 75% are in submucosa, 15% in the muscular layers, and 10% in the subserosa ( 4,5,6 ). However heterotopic pancreatic tissue may be implanted extraintestinaly. e.g.gallbladder, common bile duct, liver, spleen, omentum¸ lungs¸ umbilicus¸ mediastinum etc.
In the most cases this anomaly is an incidental finding without requiring further investigations or management. The most common clinical symptoms attributed to ectopic pancreas are abdominal (epigastric pain)¸ dyspepsia¸ and GI bleeding (7¸8 ). Pyloric obstruction by ectopic tissue¸ obstruction of the ampulla of Vater, the intestine and the biliary tree were described as well. Pancreatitis in the ectopic tissue¸ cyst formation and inflammation with necrosis of the adjacent structures has been reported (2¸3¸9 ). Several cases of cancer occurring in ectopic pancreas have been already described ( 8 ). A correlation has been established between the presence of symptoms, the size of the lesion and the extent of mucosal involvement. Clinically significant lesions are greater than 1,5cm in diameter and are adjacent to or directly involve the mucosa (7).
Pancreatic rest appears as round, smooth submucosal filling defects with a central umbilication on barium contrast studies. 80% of lesions vere located on the greater curvature in the prepyloric region, as in our patients (Figure 1a, 1b ). Endoscopically, pancreatic rest appears as a round, sometimes yellow, well defined. firm, intramural lesion from 2mm to 4cm in diameter with a central depression which may ulcerate (Figure 2a, 2b ). Histological diagnosis of abberant pancreas is usually difficult when tissue specimens are obtained using a standard endoscopic biopsy forceps. Tissue examination usually reveals normal pancreatic lobules with all pancreatic structural elements, e.g. ducts¸ acini¸ and islets of Langerhans.
Managemenet of ectopic pancreas is somewhat controversial. Because this anomaly is largely asymptomatic and rarely associated with clinical pathology¸ the incidental finding of characteristic lesion does not necessarily warrant excision. Endoscopic removal is dangerous because of risk of perforation or bleeding since the lesion is submucosal. Operative treatment is reserved for complicated cases¸ when clinical symptoms are associated with its presence such as recurrent bleeding, obstruction, or malignant degeneration or when its appearance is difficult to differentiate from the other lesions such as leiomyoma or carcinoid.
REFEREENCES
1. Grendell JH, Ermak TH. Anatomy, Histology, Embriology, and Developmental Anomalies of the Pancreas. In:Sleisenger &Fordtran's Gastrointestinal and Liver Disease, Philadelphia: WBSaunders,1998:761-71.
2. Kopelman HR. The pancreas: Congenital anomalies. In: Walker WA¸ Durie PR¸ Hamilton RJ¸ Walker-Smith JW¸ Watkins JB¸ eds. Pediatric Gastrointestinal Disease. St.Lous: Mosby¸ 1996; 1427 - 6
3. Parker HW. Congenital anomalies of the pancreas. In:Sivak MV. Gastroenterologic Endoscopy. Philadelphia:WB Saunders, 1987:770-779.
4. Masi C, Benvenuti P, Freschi G, et al. Frequency and clinical significance of ectopic pancreas. Minerva Chir 1990;45:5-10.
5. Lucandri G, Castaldo P, Meloni E, Ziparo V. Ectopic pancreas with gastric localization: a clinical case and review of the literature. G Chir 1994;15:162-6.
6. Bedossa P, Millat B, Zrihen E, Lemaigre G. Adenocarcinoma in heterotopic gastric pancreas. Gastroenterol Clin Biol 1991; 15:79-82.
7. Matsushita M, Hajiro K, Okazaki K, Takakuwa H. Gastric aberrant pancreas: EUS analysis in comparison with the histology. Gastrointest Endosc 1999;49:433-9.
8. Arao J, Fukui H, Hirayama D, et al. A case of aberrant pancreatic cancer in the jejunum. Hepatogastroenterology 1999;46:504-7.
9. Souli A, Person B, Cervi C, et al. Pseudotumor pyloric stenosis of aberrant pancreas. Press Med 1997;26:1293-4.
Table 2: Classification of Pancreatic Anomalies
1. Migration anomalies
- Anular pancreas
- Ectopic pancreas
2. Fusion anomalies
- Pancreas divisum
3. Ductal duplication anomalies
- Number variations
- Form variations
4.Miscellaneous
- Agenesis
- Hypoplasia
- Cystosis
- Pancreatic "bladder"
- True accessory pancreas
Table 1: Clinical features of patients with gastric ectopic pancreas
Case Age Gender Location Other lesions Symptoms Therapy
1. 14 F prepyloric none melaena Operation
2. 24 M prepyloric none nonspeficic Follow-up
3. 22 M prepyloric none nonspecific Follow-up
4. 20 F prepyloric none nonspecific Follow-up
Figure 1a, 1b. Barium study of the upper gastrointestinal tract demonstrating a round pancreatic rest in the antrum pyloricum.
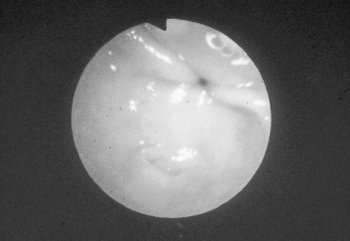
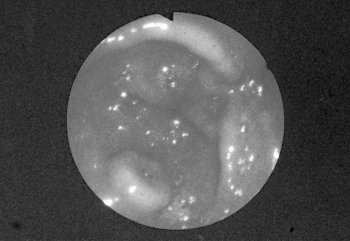
Figure 2a and 2b. Endoscopic view of the pancreatic rest : a round mucosal elevation in the antum pyloricum with the central depression,.

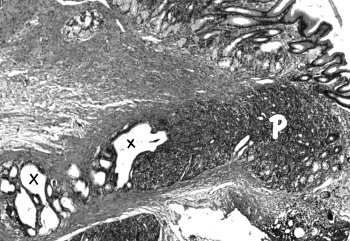
Figure 3a. Ectopic pancreas histology: note ectopic pancreatic tissue ( P ) within the gastric wall. Small pancreatic ducts ( x ) are present; one is dilated, cystic in nature Gastric glands ( arrow ) are of pyloric type.
Figure 3b. Gastric pancreatic choristoma ( P ) with dilated draining ducts ( x ). Note gastric mucosa of pyloric type.