CONJUGATED BILE ACID REPLACEMENT THERAPY
IN SHORT BOWEL SYNDROME
An American - Serbian Development
Alan F. Hofmann, M.D.
Division of Gastroenterology, Department of Medicine
University of California, San Diego
The authors work is supported by NIH Grant RO 37172 (PI: Dr. John S. Fordtran, Baylor University Medical Center), as well as a grant-in-aid from the Falk Foundation, e.V., Freiburg, Germany. The figures and tables have been published elsewhere (1).
Abstract
An intraluminal bile acid deficiency is present in most short bowel syndrome (SBS) patients and contributes to fat maldigestion. The first study done that established the efficacy of cholylsarcosine in short bowel syndrome ( SBS ) patients were done by Professor Popovic , and their findings were confirmed by American, Danish, and German studies. In SBS patients lacking a colon, natural bile acids appear to be as efficacious as cholylsarcosine because bacterial dehydroxylation does not occur. However, the clinical value of conjugated bile acid replacement in such jejunostomy patients is unclear because such patients frequently require parenteral fluid and electrolyte replacement providing an alternative and efficient route for caloric supplementation. In SBS patients with a colon, a diet rich in fermentable carbohydrate is desirable, because colonic formation of short chain fatty acids from malabsorbed carbohydrate is an important caloric source. Therefore increased efficiency of lipid absorption results in only a modest gain in calorie assimilation. We conclude that although conjugated bile acid replacement therapy is rational and unequivocally increases lipid absorption in SBS, its clinical usefulness is likely to be restricted to jejunostomy patients. Nonetheless, in such patients, conjugated bile acid replacement therapy still will not eliminate the requirement for parenteral supplementation of fluid and electrolytes. Studies are needed that compare the cost/benefit ratio of parenteral lipid administration versus the enhancement of absorption of dietary lipid by conjugated bile acid replacement therapy.
Introduction
This article will review briefly the rationale of and recent clinical data on conjugated bile acid replacement therapy in SBS patients. Conjugated bile acid replacement therapy in patients with SBS was a long standing interest of the late Obren Popovic, and his group was the first to show that cholylsarcosine, a deconjugation-dehydroxylation resistant bile acid developed in my own laboratory, would enhance lipid absorption in ileal resection patients.
An Overview of Bile Acid Metabolism
Bile acids are synthesised in the hepatocyte from cholesterol by a complex multi-enzyme process. After synthesis, bile acids are conjugated with glycine or taurine and the resulting conjugated bile acids are secreted into bile. Conjugated bile acids are efficiently absorbed from the small intestine by at least two carrier-mediated processes. The most important of these is the ileal transport system that consists of an apical sodium/conjugated bile acid co-transporter and a basolateral bile acid transporter that has not been well characterized. Bile acids return to the liver in portal venous blood, and are efficiently extracted by the liver and once again secreted into bile thus undergoing an enterohepatic circulation (2-4).
The efficient intestinal absorption of conjugated bile acids leads to the accumulation of a recycling mass of bile acids termed the bile acid pool whose mass can be estimated by an isotope dilution procedure. In man, the conjugated bile acid pool is about 2 grams in size, and cycles about twice per meal. The product of the bile acid pool times the recycling frequency gives bile acid secretion. This can be measured by an indicator dilution procedure that involves intubation of the small intestine and perfusion of a nonabsorbable marker during a normal eating pattern (5,6,7). When a meal is ingested, vagal stimulation and cholecystokinin release cause the gallbladder to contract, discharging its contents into the small intestine. Bile acid secretion is about 4 g/meal (2 gm/hour) falling to much lower values in the interprandial intervals. Bile acid biosynthesis is 200-500 mg/day (depending on the method of measurement). Thus enterohepatic cycling increases the flux of bile acids by a factor of about fifty. Between meals, the majority of the bile acid pool is stored in the gallbladder. Because the fractional hepatic extraction of bile acids returning to the liver is constant, the instantaneous flux of bile acids that is absorbed from the small intestine can be estimated approximately by the concentration of bile acids in systemic venous plasma.
Bile acid secretion is under homoeostatic control at both intestinal and hepatic levels. At an intestinal level, at least in man, bile acid feeding downregulates total ileal transport. This has not been shown experimentally, but is an inference from multiple studies showing that bile acid feeding does not cause increased bile acid secretion (7,8). In the guinea pig, administration of a bile acid sequestrant, which lowers the intraluminal bile acid concentration, upregulates ileal bile acid transport (9). Whether such occurs in man is not known. Against this simple negative feedback control of ileal transport by intraluminal bile acid concentration are other observations that suggest there may be positive feedback. For example, in the rat, biliary diversion (10) or bile duct ligation (11) cause marked down regulation of ileal transport; and cholic acid feeding results in upregulation of ileal transport (12). Similarly, in the pig, parenteral nutrition results in a marked reduction in bile acid transport by the ileum (13).
At a hepatic level, bile acid synthesis appears to be regulated directly or indirectly by the intrahepatocyte concentration of bile acids (14). In most species including man, interruption of the enterohepatic circulation by biliary diversion, bile acid sequestrant administration, or ileal resection results in increased bile acid biosynthesis (14). Conversely, bile acid feeding, at least in man, results in downregulation of bile acid biosynthesis (7,8,14).
In the healthy human, bile acid biosynthesis is downregulated. Bile acid feeding decreases bile acid biosynthesis by 50%, but interruption of the enterohepatic circulation generally results in a ten to twenty fold increase in bile acid biosynthesis (4).
The Role of Bile Acids in Lipid Digestion and Absorption
Pancreatic lipase hydrolyses dietary triglyceride to 2-monoacylglycerol (2-monoglyceride) and fatty acid. The 2-monoglyceride and fatty acid are insoluble in intestinal content and form a hydrated liquid crystalline phase of multiple bilayers on the surface of the lipid droplets. Conjugated bile acid molecules adsorb to this liquid crystalline phase and if the concentration of bile acids is sufficiently high, the phase is transformed to a micellar phase (15). The micelles are believed to be cylindrical; the monoglyceride and fatty acid molecules are arranged in a cylinder with the polar head groups facing outward. The bile acid molecules are present between the polar head groups, the hydrophilic side of the bile acid molecule facing the aqueous phase surrounding the mixed micelle (16,17). The shape of the bile acid molecule appears to be more important than its anionic charge as a zwitterionic bile acid (CHAPS) also transforms lipid bilayers into cylindrical micelles.
Micellar solubilization increases the aqueous concentration of fatty acid and monoglyceride by several orders of magnitude. Estimates of the aqueous solubility of long chain fatty acids such as palmitic and stearic have suggested that such molecules are virtually insoluble at physiological pH (18). Although the micelle diffuses more slowly than individual molecules, the overall diffusive flux is enhanced by at least a hundred fold by micellar solubilization (19). Micellar solubilization thus enhances diffusion of insoluble lipids through the unstirred layer of water coating the surface of the small intestine. Even though the thickness of this layer is less than previously believed (20), diffusion is still likely to be rate limiting in the absorption of long chain fatty acids because transmembrane flipflop of fatty acids is extremely rapid (21).
Micellar solubilization by conjugated bile acids also enhances the absorption of other key dietary lipids such as fat-soluble vitamins. Until recently, it was believed that the sole function of bile acids was to serve as a solvent sink for such molecules; uptake was considered to occur from either from the low concentration of lipids in monomeric form or by collision of the micelle with the lipid layer of the apical membrane of the enterocyte. However, new studies (22,23) have indicated that bile acids differ in their ability to promote cholesterol absorption, raising the possibility of some type of interaction between the mixed micelle and one or more membrane transporters involved in the uptake of insoluble lipids. The scavenger receptor SRB2 has been proposed as a transporter involved in cholesterol absorption (24).
Intraluminal deficiency in short bowel syndrome
Most patients with SBS have undergone ileal resection. In patients with extensive ileal resection, a bile acid deficiency is present in the small intestine (25-27). The intraluminal concentration declines progressively during the day whereas in healthy subjects, bile acid secretion differs little during consecutive equicaloric meals (25). A bile acid deficiency is present in ileal resection patients because maximal bile acid synthesis -- 4-6 gm/day -- is less than bile acid secretion when the enterohepatic circulation is intact. Moreover, the compensatory increase in bile acid synthesis is not identical in all ileal resection patients, and in some patients bile acid synthesis may increase only slightly.
There do not appear to be any measurements for intraluminal bile acid concentrations in SBS patients. Bile acid secretion can be expected to be greatly reduced if severe bile acid malabsorption if present. Moreover if jejunal secretion of water and electrolytes is increased in SBS, as has been reported (28), bile acid concentrations will be further reduced.
In patients with SBS, the severe fat malabsorption that is present is likely to result from three factors: decreased intraluminal bile acid concentration, decreased mucosal surface area, and decreased exposure time because of rapid small intestinal transit time. Of these, decreased surface area and decreased exposure time are likely to be most important. In patients with biliary obstruction or diversion, fatty acids can be absorbed by recruitment of the ileum, which serves as an anatomical reserve (29). In the absence of micelle formation, fatty acid solubility is likely to determine the extent of absorption. Medium chain fatty acids are water soluble and well absorbed in the absence of bile acids (30). When fat malabsorption is induced by cholestyramine administration, the extent of fatty acid malabsorption is directly proportional to chain length for fatty acids. The longer the chain length, the greater the degree of malabsorption (31).
It is well known that small intestinal transit is extremely rapid in SBS in part because of increased gastric and jejunal secretion. In addition, the absence of the ileum leads to loss of the ileal brake which is considered to slow jejunal transit (32). To improve lipid absorption in SBS, one should restore the bile acid concentration to micellar levels, induce maximal hypertrophy and hyperplasia of the remaining small intestine, and decrease the rate of small intestinal transit. Obviously, correcting the bile acid deficiency is only a partial solution. From a pathophysiological standpoint, however, the extent to which fat absorption is improved by bile acid replacement therapy defines the contribution of bile acid deficiency to fat malabsorption.
Conjugated bile acid replacement therapy: prior studies
At the turn of the century, the precise role of bile acids in promoting lipid absorption was not understood, although from the experiments of Claude Bernard in the rabbit, it was clear that bile acids played a role in promoting lipid absorption (33). A careful balance study in a bile fistula patient, performed nearly a century ago, showed that bile acids appeared to enhance lipid absorption and improve nutrition (34). In the discussion of the paper, the authors note that the European view is that oral bile preparations have no therapeutic value. In the pharmacy textbooks of that time, bile acids are not listed as therapeutic agents. Moore and Rockwood isolated a clear phase containing solubilized fatty acids from human intestinal content by centrifugation (35), and they as well as Wieland and Sorge (36) proposed that bile acids somehow formed polymolecular complexes with fatty acids. Henrik Dam (37) discovered vitamin K (K for Koagulation), A few years later, Hugh Butt and his colleagues at the Mayo Clinic in a groundbreaking study reported the first successful correction of a vitamin K deficiency in a patient with biliary obstruction (and intraluminal bile acid deficiency). Butt and his colleagues showed that a crude vitamin K preparation was absorbed and effective only when given together with conjugated bile salts (38). This study stimulated the development of water-soluble vitamin K analogues that are used today for correction of clinical states of vitamin K deficiency.
In the late 1940's Annegers at Northwestern University showed that replacement of bile to dogs with biliary diversion caused a considerable increase in lipid absorption (39). This study may have led to the marketing of ox bile salts by the Eli Lilly Company, but there is no evidence that controlled studies documenting efficacy and safety were ever performed in man.
In 1960, Lack and Weiner (40) reported that the ileum actively transported conjugated bile acids, thus providing for the first time a mechanism for intestinal conservation of conjugated bile acids. Perfusion studies confirmed that the ileum was the major site of conjugated bile acid replacement in ma (41). At the same time, the role of conjugated bile acids in enhancing lipid absorption was finally clarified by showing that conjugated bile acids form mixed micelles with fatty acids and monoglycerides in vitro (42), and that a micellar phase could be isolated from small intestinal content during fat digestion (43).
The finding that the ileum was the major site of bile acid conservation prompted studies in patients that had undergone ileal resection. A study in an SBS patient lacking an ileum confirmed that bile acid malabsorption and an intraluminal bile acid deficiency were present. However, an attempt to increase lipid absorption by desiccated sheep bile did not give encouraging results (44). At about the same time, Hardison and Rosenberg showed that ileal resection patients had bile acid malabsorption. They administered a crude bile salt preparation and found that although it improved lipid absorption, it worsened the diarrhea in some of the patients (45).
An explanation for diarrhea induced by exogenous bile salt administration was provided by the Mayo group who showed using the colonic perfusion technique that dihydroxy bile acids, whether conjugated or unconjugated, induced colonic secretion and caused histological evidence of mucosal injury (46,47). Clinical studies also performed at the Mayo Clinic showed that bile acid sequestrant administration decreased or \abolished the diarrhea present in some ileal resection patients (48). Thus, the conclusion emerged that although conjugated bile acids enhance lipid absorption by micellar solubilization, they also induce colonic secretion when present in the colon at abnormally high concentrations. Therefore, any attempt to correct an intraluminal bile acid deficiency by oral bile acid ministration was likely to induce diarrhea, and this undesirable side effect would probably outweigh any improvement in caloric assimilation.
Also, at this time, medium chain triglycerides were introduced into clinical medicine, largely through the efforts of Vigen Babayan (49). These semisynthetic triglycerides were composed of esterified fatty acids ranging from C8 to C12 to in length. They were rapidly hydrolysed by pancreatic lipase; the liberated fatty acids were water soluble and efficiently absorbed. Absorption is now known to occur by both transcellular and paracellular pathways (50), with little esterification occurring during transport. The medium chain fatty acids are not incorporated into chylomicrons but are absorbed via portal venous blood. The fatty acids were taken up by the liver and rapidly oxidised in the mitochondria (51).
The diarrhea induced by oral conjugated bile salt administration should not occur in a patient with SBS lacking a colon. Fordtran and his colleagues reported enhance lipid absorption in an SBS patient lacking a colon in 1973 (52), an observation confirmed by the Popovic group some 15 years later (53). Later, the Fordtran group extended these studies by reporting that ox bile salt administration to a patient with some residual colon increased lipid absorption without causing an increase in diarrhea (54).
Development of cholylsarcosine, a deconjugation-dehydroxylation resistant, non-secretory bile acid:
In San Diego, in the late 1980's, we returned to the problem of identifying a suitable conjugated bile acid replacement molecule. Studies by Suzie Huighebaert in our laboratory had shown the chemical structure of the amino acid is a key determinant of the susceptibility of N-acyl amidates (conjugates) of bile acids to deconjugation by cholylglycine hydrolase (55). At about the same time, Batta and his colleagues showed that cholylsarcosine was resistant to deconjugation by cholylglycine hydrolase (56). This suggested to us that all sarcosine conjugates of bile acids might be resistant to bacterial deconjugation. To test the validity of this concept, we performed a study in collaboration with the group of the late Erwin Mosbach (57). Rabbits were fed ursodeoxycholic acid (UDCA) conjugated with glycine or taurine or with the N-methyl derivatives of these compounds. Rabbits receiving the taurine and glycine amidates of UDCA showed the expected enrichment of lithocholic acid in bile with associated hepatotoxicity. The lithocholic acid had been formed from the UDCA glycine and taurine amidates by bacterial deconjugation and 7-dehydroxylation. In contrast, animals receiving the N-methyltaurine and N-methylglycine (sarcosine) amidates of UDCA showed neither an increased proportion of lithocholic acid in biliary bile acids nor histological evidence of liver injury. These experiments indicated that sarcosine conjugates of bile acids were resistant to bacterial deconjugation and dehydroxylation in vivo.
Cholylsarcosine was selected as a potential bile acid replacement molecule. Cholic acid is not secretory except at very concentrations in the perfused colon (46,47), and is relatively non-cytotoxic when incubated with isolated hepatocytes (58,59) and mast cells (60). It is available at relatively low cost. Sarcosine has no toxicity, as evidenced by the lack of phenotypic manifestations of sarcosinemia, an inborn error of sarcosine metabolism.
Adrian Schmassmann showed that cholylsarcosine was resistant to deconjugation-and dehydroxylation in three rodent species. The compound was well transported by the liver and the ileum (60). Jan Lillienau working with Claudio Schteingart defined the physicochemical properties of cholylsarcosine. These properties are summarized in Table I. These workers showed that the physicochemical properties of cholylsarcosine differed little from cholylglycine (glycocholate). They showed that cholylsarcosine enhanced triglyceride lipolysis as well as cholyltaurine (taurocholate) and that cholylsarcosine and cholyltaurine promoted triglyceride absorption similarly when a triglyceride emulsion was perfused into the intestine of a lymph fistula rat. Lillienau et al showed that cholylsarcosine was non-secretory in the perfused rabbit ileum (62). The metabolism of cholylsarcosine in the rat is summarized in Table 2.
To test the efficacy of cholylsarcosine as a conjugated bile acid replacement molecule, Sarah Longmire-Cook et al resected the distal third of the small intestine in two dogs, thereby creating an animal preparation simulating SBS. The dogs had severe fat malabsorption that was markedly decreased in a dose-related manner when cholylsarcosine was added to their diet (63).
These experiments suggested that cholylsarcosine had all of the desired properties of a conjugated bile acid replacement molecule. Schmassmann, working with his Swiss colleagues showed that in man, the Tmax for ileal transport of cholylsarcosine differed little from that of cholylglycine, and that cholylsarcosine had no apparent hepatotoxicity when being absorbed at the maximal ileal transport rate (64). Studies of Schmassmann also showed that the effect of cholylsarcosine on bile flow and biliary secretion differed little from that of cholylglycine. The physiological properties of cholylsarcosine in humans are summarized in Table 3.
To test whether cholylsarcosine possessed any hepatotoxic properties, studies were performed in patients with primary biliary cirrhosis who had responded incompletely to ursodeoxycholic acid (UDCA) alone. Cholylsarcosine was coadministered together with UDCA. This study, performed at the Mayo Clinic by Ricci and Lindor (65), showed that the addition of cholylsarcosine to UDCA caused no change in liver tests. Thus, in this cholestatic disease in which bile acids accumulate in the hepatocyte, cholylsarcosine was devoid of apparent hepatotoxicity.
Together these studies suggested that cholylsarcosine was safe and should be effective as a conjugated bile acid replacement molecule in conditions associated with an intraluminal deficiency of conjugated bile acids.
Clinical Trials of Cholylsarcosine as conjugated bile acid replacement therapy:
Pharmaceutical formulation of cholylsarcosine: The Falk Foundation e.V. in Freiburg kindly commissioned the synthesis of a 5 kg lot of cholylsarcosine by the Diamalt Company (now Goodrich Chemical Company), under the supervision of Dr. Thilo Messerschmidt. The material was formulated in microcapsules coated with a pH sensitive coating that would dissolve above pH 6. The rationale for this formulation was as follows. The size of the particles had to be less than 2 mm in diameter so that they would empty from the stomach with the meal. They should not dissolve in gastric content but should dissolve rapidly in duodenal content. The required dose was thought to be 4 gm/meal. Because cholylsarcosine dissolves above pH 3.7, and because gastric pH frequently increases to this level during digestion of a meal, it was feared that high concentrations of cholylsarcosine would occur in the stomach and would enter the gastric mucosa in protonated form causing severe mucosal damage. Gastric damage by micellar concentrations of cholyltaurine (taurocholate) is well described in the literature (66).
Clinical experience with cholylsarcosine as bile acid replacement therapy: The first clinical trial using this material was performed by Obren Popovic and his colleagues in Belgrade. Results were discouraging (67). The patients showed abdominal pain or increased diarrhea. Professor Popovic informed me of his discouraging findings by a letter in 1994. It was not clear to me why cholylsarcosine did not work, but I considered the results of this therapeutic trial to be valid in part because of the experience of this group with conjugated bile acid replacement therapy.
Then Professor Popovic had the idea that perhaps the lack of efficacy and the undesirable side effects of cholylsarcosine were not due to the material per se, but the failure of the enteric coating to dissolve. This idea was not unreasonable because of the rapid transit time that is frequently present in such patients. Professor Popovic obtained the pure chemical in powder form from the Falk Foundation, and packaged it in gelatine capsules. He then treated two ileal resection patients and found that steatorrhea decreased in both of the patients, and that diarrhea decreased in one of them. He wrote me of his remarkable findings in a letter in 1995 and his findings were published in early 1998 (68).
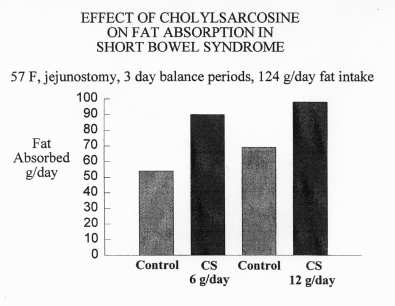
In 1997, Dr. John Fordtran of the Baylor University Medical Center in Dallas, Texas, contacted me to find out whether I had a conjugated bile acid that I might supply for him to be used in a patient with SBS. The patient had undergone several intestinal resections and was left with only a small segment of jejunum that ended in a jejunal stoma. Parenteral nutrition had been discontinued because of a brachio-cephalic clot, and medium chain triglycerides were not tolerated. Jejunostomy output averaged 3000 gm/day and there was severe steatorrhea (100 gm/day). The patients weight had declined to 41 kg and she was despondent.
The reason for Dr. Fordtrans contacting me was his inability to obtain an ox bile salt preparation that had previously been marketed by the Eli Lilly Company and was no longer available. I provided cholylsarcosine (the preparation prepared by the Diamalt Company) to Dr. Fordtran who, together with his research fellow, Dr. Christine Gruy-Kapral and his research team, performed a careful balance study. The patient was fed a repeating diet. Periods were four days in length, and a variety of measurements were made on the fecal output (from the jejunostomy bag). The dose of cholylsarcosine used was 6 gm/day or 12 gm/day. While this work was in progress, Dr. Gruy-Kapral learned of an Austrian company, Neuber that sold an extract of ox bile containing mostly conjugated bile acids. The material was prepared by the addition of alcohol and charcoal to crude ox bile followed by filtration after over night incubation in the cold. The filtrate was taken to dryness giving a powder that by enzymatic and high pressure liquid chromatographic (HPLC) analysis, consisted of 90% conjugated bile salts predominantly cholylglycine and cholyltaurine. A second balance study was performed in which the replacement bile acid material was the conjugated bile acid mixture (mixed ox bile salts); the identical dose of bile acid was used.
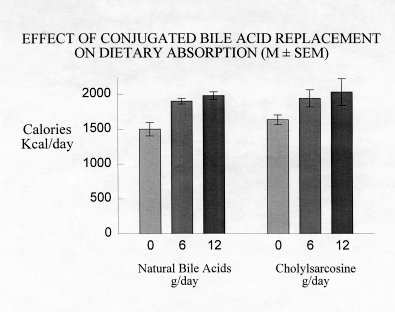
The results of these studies were remarkable (69). Cholylsarcosine and the mixed ox bile salts each caused a 50% increase in fat absorption at a dose of 2 gm/meal or 6 gm/day. Increasing the dose to 12 gm/day caused only a slight increase in fat absorption. There was no difference whatsoever between the results with cholylsarcosine and the mixed ox bile salts. Bomb calorimetry of feces was performed. The reduction in caloric output could be accounted for solely by the decreased fat output. Thus, cholylsarcosine and the ox bile salts caused enhanced absorption of fat, but did not affect the absorption of carbohydrates or proteins. Both agents caused increased Ca2+ absorption, but the absorption of no other dietary constituent was influenced by bile acid replacement. Fecal weight did not change.
Because of these encouraging results, the patient was discharged and advised to continue to ingest the ox bile salt preparation at home at a dose of 2 gm/meal. Over the next six months, the patient gained 15 pounds, and is now happy with her physical appearance.
In May 1998, Professor Per Brobech Mortensen visited my laboratory, Professor Brobech Mortensen has had a longstanding interest in the SBS, and he and his colleague Jeppesen have performed meticulous balance studies defining the role of the colon in caloric input in SBS patients (70). More recently, they have defined exactly what is the minimal level of gut function that allows an SBS patient to avoid parenteral nutrition (71). Brobech Mortensen performed a balance study comparing two doses of cholylsarcosine in 4 SBS patients, 2 with a colon and 2 without a colon. (Cholylsarcosine was prepared by an Italian company, Prodotti Chimici e Alimentari S.p.A,). In all patients, increased lipid absorption was obtained. In one patient with a colon, diarrhea increased. Another patient had severe gastric irritation when ingesting cholylsarcosine and had to be withdrawn from the study (72).
Brobech Mortensen performed gas liquid chromatography of fecal fatty acids to determine which fatty acids had their absorption enhanced by cholylsarcosine. He found that the longer the chain length, the greater was the enhanced absorption. Thus, cholylsarcosine increased the absorption of palmitic (C16 ) and stearic (C18 ) to a much greater extent than that of oleic acid (C18, but with one double bond) or dodecanoic (C12) (72).
Jürgen Stein, Wolfgang Caspary and their associates at the University of Frankfurt, Germany, performed another clinical study. Increased lipid absorption was observed in all patients, whether or not a colon was present. Two patients developed gastric irritation manifested by nausea and/or vomiting (73).
Results of these clinical trials are summarized in Table 4. .
The side effects of cholylsarcosine appear to be related to excessive bile acid concentrations in either the stomach or the colon. The increased diarrhea observed in one of Brobech Mortensens patients could be caused either by a secretory effect of cholylsarcosine per se, or by a secretory effect of micellar fatty acid in the colon. Fatty acids are known to have secretory effects in the perfused human colon (74).
The results of these studies now totalling some 14 patients indicate that cholylsarcosine increases lipid absorption, especially of hydrophobic fatty acids. Side effects are restricted to gastric or colonic irritation. Unfortunately, the magnitude of this effect is sufficient to preclude therapy, at least with neat material packaged in gelatine capsules in some patients.
The Questionable Importance of conjugated bile acid replacement in SBS:
The question is whether these findings indicate that cholylsarcosine is an important advance in the management of SBS patients. The subsequent discussion suggests that the clinical usefulness of cholylsarcosine is not yet certain.
Cholylsarcosine in the management of jejunostomy patients:
SBS patients lacking a colon are more likely to require parenteral nutrition than SBS patients possessing a colon (71,75) are. Danish studies suggest that parenteral nutrition is required when either fluid assimilation is less than the minimal daily water requirement (1000-1500 ml/day) or caloric assimilation is less than the minimal energy expenditure (25-35 kcal/kg/day) (71). The failure to absorb water is related in part to increase gastric and jejunal secretion (28) and in part to the rapid transit and decreased mucosal surface area. Increased gastric secretion can be abolished with protein pump inhibitors, but no satisfactory treatment for increased jejunal secretion has been proposed.
If parenteral fluid must be given to maintain water and electrolyte balance, then it is relatively easy to add lipid calories to the infusion mixture. The study of Gruy-Capral et al (69) suggested that mixed bovine bile salts and cholylsarcosine had identical efficacy in promoting lipid and calcium absorption. Since dehydroxylation of bile acids does not occur in such patients, there is no obvious benefit to giving a dehydroxylation resistant conjugated bile acid analogue. Some jejunostomy patients maintain adequate caloric assimilation by hyperphagia (71). Conjugated bile acid replacement could decrease the requirement for hyperphagia but whether patients would prefer to overeat or eat less and take capsules during a meal is problematic. There can be occasional patients like the one described by Gruy-Kapral et al for whom conjugated bile acid replacement caused a meaningful improvement in caloric assimilation and desirable weight gain.
The bottom line is, in my opinion, that the physician should attempt to judge whether increased efficiency of dietary fat and calcium would benefit his or her patient. If there is any doubt, a therapeutic trial of natural conjugated bile acids or cholylsarcosine is indicated. At present, neither preparation is readily available, but this situation is likely to change in the future. Perhaps natural conjugated bile acid mixtures can be marketed as dietary supplements, bypassing the complex and expensive regulatory process required for ethical drugs.
Cholylsarcosine in the management of SBS patients possessing a colon:
In SBS patients with a colon, colonic fermentation of malabsorbed carbohydrate by anaerobic bacteria generates short chain fatty acids that are an important caloric source (70). Because of this colonic salvage, as noted above, SBS patients with a colon are less likely to require parenteral nutrition (71,75). If such patients ingest a diet rich in fermentable carbohydrate, the proportion of lipid calories in the diet will be correspondingly reduced. Therefore although the fractional absorption of lipid can be increased by cholylsarcosine administration, it remains unclear whether the magnitude of increased caloric absorption is sufficient to justify the cost of the compound. A second problem is that in such patients, administration of cholylsarcosine results in a micellar phase containing fatty acid in the colon. There is no evidence to date suggesting that colonic absorption of such solubilized fatty acid is appreciable. If the colonic epithelial cell were to adapt to an increased absorptive flux of fatty acids and begin to make chylomicrons, the colonic salvage of malabsorbed lipids would occur, and thereby provide a rationale for cholylsarcosine. However, this seems unlikely to occur. Moreover the unequivocal increase in fecal weight observed in one of Brobech Mortensens patients (72), suggests that the solubilized fatty acid may induce colonic secretion of water. Thus, although the idea of conjugated bile acid replacement is rational in such patients, it appears that the benefit is small because the diet is low in lipids and also because a micellar phase of fatty acid in the colon may have undesirable effects. The total number of SBS patients possessing a colon that have been studied is quite small, and it may be that there is considerable variation in clinical response.
Epilogue: The problem of bile acid deficiency has now been solved, but it does not appear that the solution (cholylsarcosine or natural conjugated bile acids) is a major clinical advance. The need for the key function of conjugated bile salts to enhance the absorption of fat-soluble vitamins and very hydrophobic fatty acids can be circumvented by giving the compounds parenterally. Medium chain triglycerides do not require bile acids for absorption, and water-soluble derivatives of vitamins K and E have been developed. It seems desirable to test whether re-establishment of a micellar phase has other effects for example binding of endotoxin or prevention of bacterial translocation. There is likely to be an occasional in SBS patient with a jejunostomy in whom conjugated bile acid replacement therapy will provide a sufficient increment in caloric absorption so as to be clinically useful.
Obren Popovic did not live to see his results confirmed, but his colleagues should take pleasure in that he pioneered in a new adventure in the therapy of digestive disease.
Acknowledgements: The author acknowledges invaluable correspondence with Per Brobech Mortensen, University of Copenhagen, who is responsible for many of the ideas developed here. He also acknowledges the continued stimulation of Dr. John Fordtran and his colleagues at the Baylor University Medical Center in Dallas, Texas. The author also acknowledges the help of his fellows and colleagues who have contributed to the development of cholylsarcosine as a replacement bile acid. Key contributions were made by Adrian Schmassmann, Jan Lillienau, Sarah-Longmire Cook, Claudio Schteingart, Huong-Thu Ton-Nu, and Lee Hagey. Others who contributed in his laboratory were Sam Marcus, Rudy Danzinger, Oliver Esch, Steve Rossi, and Young Kim. Collaborators included Bertram Cohen, Erwin Mosbach (now deceased), Doug Heuman, Reno Vlahcevic, Phil Hylemon, Michael Pandak, Paola Ricci, and Todd Stravitz. . The Falk Foundation e.V., Freiburg, Germany generously provided the first bulk material. A patent was issued in 1992 to the University of California for the use of cholylsarcosine as a bile acid replacement molecule, but the patent was not licensed and has now expired.
REFERENCES
1. Hofmann AF, Conjugated bile acid replacement therapy for enhanced lipid absorption in bile acid deficiency states. In: Christophe A, ed. Fat Digestion and Absorption, Champaign IL: AOCS Press, 2000; in press.
2. Carey MC, Duane WC, Enterohepatic circulation. In: Arias IM, Boyer JL, Fausto N, Jakoby WB, Schachter D, Shafritz DA, eds. The Liver: Biology and Pathobiology, (Third Edition). New York: Raven Press, 1994; 719-767.
3. Hofmann AF, Biliary secretion and excretion: the hepatobiliary component of the enterohepatic circulation of bile acids. In: Johnson LR, Alpers DH, Christensen J, Jacobson ED, Walsh JH, eds. Physiology of the Gastrointestinal Tract, Third Edition, volume 2. New York: Raven Press, 1994; 1555-76.
4. Hofmann AF, Intestinal absorption of bile acids and biliary constituents: the intestinal component of the enterohepatic circulation and the integrated system. In: Johnson LR, Alpers DH, Christensen J, Jacobson ED, Walsh JH, eds. Physiology of the Gastrointestinal Tract, Third Edition, volume 2. New York: Raven Press, 1994; 1845-65.
5. Brunner H, Northfield TC, Hofmann, AF, Go VLW, Summerskill, WHJ: Gastric emptying and secretion of bile acids, cholesterol, and pancreatic enzymes during digestion: duodenal perfusion studies in healthy subjects. Mayo Clin Proc 1974: 49; 851-60.
6. Northfield TC, Hofmann AF: Biliary lipid output during three meals and an overnight fast. I. Relationship to bile acid pool size and cholesterol saturation of bile in gallstone and normal subjects. Gut 1975:16:1-11.
7. LaRusso NF, Hoffman NE, Hofmann AF, Northfield TC, Thistle JL: Effect of primary bile acid ingestion on bile acid metabolism and biliary lipid secretion in gallstone patients. Gastroenterology 1975; 69: 1301-14.
8. Von Bergmann K, Epple-Guttsfeld M, Leiss O: Differences in the effects of chenodeoxycholic and ursodeoxycholic acid on biliary lipid secretion and bile acid synthesis in patients with gallstones. Gastroenterology 1984; 87: 136-43.
9. Lillienau J, Munoz J, Longmire-Cook S, Hagey LR, Crombie DL, Hofmann AF: Negative feedback regulation of the ileal bile acid transport system in rodents. Gastroenterology 1993; 104: 38-46.
10. Higgins JV, Paul JM, Dumaswala R, Heubi JE: Downregulation of taurocholate transport by ileal BBM and liver BLM in biliary-diverted rats. Am J Physiol 1994; 267: G501-7.
11. Sauer P, Stiehl A, Fitscher BA, Riedel H-D, Benz C, Kl`ters-Plachky P, Stengelin S, Stremmel W, Kramer W: Downregulation of ileal bile acid absorption in bile duct ligated rats. J. Hepatol 2000; in press.
12. Stravitz RT, Sanyal AJ, Pandak WM, Vlahcevic ZR, Beets JW, Dawson PA: Induction of sodium-dependent bile acid transporter messenger RNA, protein, and activity in rat ileum by cholic acid. Gastroenterology 1997; 113: 1599-608.
13. Matsumura JS, Greiner MA, Nahrwold DL, Dawes LG: Reduced ileal taurocholate absorption with total parenteral nutrition. J Surg Res 1993; 54: 517-22.
14. Vlahcevic ZR, Pandak WM, Stravitz RT, Regulation of bile acid biosynthesis. In: Cooper, AD, ed. Bile Salts: Metabolic, Pathologic, and Therapeutic Considerations. Gastroenterol Clinics North Am 1999; 28:1-25.
15. Borgstr`m, B, Patton, JS, Luminal events in gastrointestinal lipid digestion. In: Schultz SG, Field M, Frizzell RA, Rauner, BB, eds. Handbook of Physiology: Section on the Gastrointestinal System, (vol. 4), Bethesda, MD: American Physiological Society, 1991; 475-504.
16 Hjelm RP Jr, Schteingart CD, Hofmann AF, Sivia DS: Form and structure of self-assembling particles in monoolein bile salt mixtures. J Phys Chem. 1995; 99: 16395-16400.
17. Hjelm RP, Schteingart CD, Hofmann AF, Thiyagarajan P: The structure of conjugated bile salt-fatty acid-monoglyceride mixed colloids: studies by small angle neutron scattering. J Phys Chem 2000; in press.
18. Vorum H, Brodersen R, Kragh-Hansen U, Pedersen AO: Solubility of long-chain fatty acids in phosphate buffer at pH 7.4. Biochim Biophys Acta 1992; 1126: 135-42.
19. Hofmann AF, Fat digestion: the interaction of lipid digestion products with micellar bile salt solutions. In: Rommel K, Goebell H, eds. Lipid Absorption: Biochemical and Clinical Aspects. Lancaster: MTP Press, 1976; 3-18.
20. Strocchi A, Corazza G, Furne J, Fine C, Di Sario A, Gasbarrini G, Levitt MD: Measurements of the jejunal unstirred layer in normal subjects and patients with celiac disease. Am J Physiol 1996; 270: G487-91.
21. Hamilton JA. Fatty acid transport: difficult or easy? J Lipid Res 1998; 39: 467-81.
22. Wang X, Hofmann AF, Tso P: Inhibition of cholesterol absorption by sodium ursodeoxycholyl taurine. Gastroenterology 1995; 108; A1196 (abstract).
23. Wang DQ-H, Tazuma S, Cohen DE, Carey MC: Natural hydrophilic bile acids profoundly inhibit intestinal cholesterol absorption in mice. Hepatology 1999; 30: 939A (abstract)
24. Hauser H, Dyer JH, Nandy A, Vega MA, Werder M, Bielauskaite E, Weber FE, Compassi S, Gemperl, A, Boffelli D, Wehrli E, Schulthess G, Phillips MC: Identification of a receptor mediating absorption of dietary cholesterol in the intestine. Biochemistry 1998; 37: 17843-50.
25. Poley JR, Hofmann AF: Role of fat maldigestion in pathogenesis of steatorrhea in ileal resection. Fat digestion after two sequential test meals with and without cholestyramine. Gastroenterology 1976; 71: 38-44.
26. Austad WI, Lack L, Tyor MP: Importance of bile acids and of an intact distal small intestine for fat absorption. Gastroenterology 1967; 52: 638-44.
27. McLeod GM, Wiggins HS: Bile salts in small intestinal contents after ileal resection and in other malabsorption syndromes. Lancet 1968; 1: 873-6.
28. Nightingale JMD, Lennard-Jones JE, Walker ER, Farthing MJG: Jejunal efflux in short bowel syndrome. Lancet 1990; 336: 765-8.
29. Knoebel LK: Intestinal absorption in vivo of micellar and nonmicellar lipids. Amer J Physiol 1972; 223; 255-261.
30. Greenberger N, Rodgers JB, Isselbacher, KJ: Absorption of medium and long chain triglycerides: factors influencing their hydrolysis and transport. J Clin Invest 1966; 45: 217-227.
31. Harkins RW, Hagerman LM, Sarrett HP: Absorption of dietary fats by the rat in cholestyramine-induced steatorrhea. J Nutr 1965; 87: 85-92.
32. Lin HC, Zhau XT, Wang L: Intestinal transit is more potently inhibited by fat in distal (ileal brake) than in the proximal (jejunal brake) gut. Dig Dis Sci 1997; 42: 19-25.
33. Bernard C: Pancreatic juice and its role in the phenomena of digestion. Medical Classics 1938; 3: 600-17.
34. Pfaff F, Balch AW: An experimental investigation of some of the conditions influencing the secretion and composition of human bile. J Exper Med 1897; 2: 49-105.
35. Moore B, Rockwood DP: On the mode of absorption of fats. J Physiol 1897; 21: 58-84.
36. Wieland H, Sorge H: Untersuchungen hber die Gallens@uren. II. Mitteilung. Zur Kenntnis der Choleins@ure. Z Physiol Chem 1916; 97: 1-27.
37. Dam H, Sch`nheyder: The occurrence and chemical nature of vitamin K. Biochem J 1936; 30: 897-901.
38. Butt HR, Snell AM, Osterberg AE: The preoperative and postoperative administration of vitamin K to patients having jaundice. J Am Med Assoc 1939; 113: 383-9.
39. Annegers JH: Function of pancreatic juice and of bile in assimilation of dietary triglycerides. Arch Int Med 1954; 93: 9-22.
40. Lack L, Weiner IM: In vitro absorption of bile salts by small intestine of rats and guinea pigs. Am J Physiol 1961; 200: 313-7.
41. Borgstr`m B, Lundh G, Hofmann AF: The site of absorption of conjugated bile salts in man. Gastroenterology 1963: 45: 229-238.
42 Hofmann AF: The role of bile salts in fat absorption: the solvent properties of dilute micellar solutions of conjugated bile salts. Biochem J 1963; 89: 57-78.
43. Hofmann AF, Borgstr`m B: The intraluminal phase of fat digestion in man: the lipid content of the micellar and oil phases of intestinal content obtained during fat digestion and absorption. J Clin Invest 1964; 43: 247-257.
44. Hofmann AF, Grundy SM: Abnormal bile salt metabolism in a patient with ileal resection. Clin Res 1965; 13: 254 (abstract).
45. Hardison WGM, Rosenberg IH: Bile salt deficiency in the steatorrhea following resection of the ileum and proximal colon. New Engl J Med 1967; 277: 337-43.
46. Mekhjian HS, Phillips SF, Hofmann AF: Colonic secretion of water and electrolytes induced by bile acids: perfusion studies in man. J Clin Inv 1971; 50: 1569-77.
47. Chadwick VS, Gaginella TS, Carlson GL, Debognie JC, Phillips SF, Hofmann AF. Effect of molecular structure on bile acid-induced alterations in absorptive function, permeability, and morphology in the perfused rabbit colon. J Lab Clin Med 1979; 94: 661-74.
48. Hofmann AF, Poley JR: Cholestyamine treatment of diarrhea associated with ileal resection. NewEngl J Med 1969; 281: 397-402.
49. Senior JR. Medium Chain Triglycerides. Philadelphia: Univ Pennsylvaia Press, 1968.
50. Amelsberg A, Schteingart CD, Stein J, Simmonds WJ, Sawada GA, Ho NFH, Hofmann AF: Intestinal absorption of dodecyl sulfate in the rodent: evidence for paracellular absorption Amer J Physio 1994; 272: G498-G506.
51. Scheig R. Hepatic metabolism of medium chain fatty acids. In: Senior JR, ed. Medium Chain Triglycerides. Philadelphia: University of Pennsylvania Press, 1968; 39-50.
52. Fordtran JS, Bunch F,Davis GR: Ox bile treatment of severe steatorrhea in an ileectomy-ileostomy patient. Gastroenterology 1973; 82: 564-568.
53. Djurdjevic D, Popovic O, Necic D, Hranisavljevic S: Ox bile treatment of severe steatorrhea in a colectomy and illeectomy patient. Gastroenterology 1973; 95: 1160 (Letter to the Editor).
54. Little KH, Schiller LR, Bilhartz LE, Fordtran JS: Treatment of severe steatorrhea with ox bile in an illeectomy patient with residual colon. Dig Dis Sci 1992; 37: 929-33.
55. Huijghebaert S.W, Hofmann AF: Influence of the amino acid moiety on deconjugation of bile acid amidates by cholylglycine hydrolase or human fecal cultures. J Lipid Res 1986; 27: 742-52.
56. Batta AK, Salen G, Shefer S: Substrate specificity of cholylglycine hydrolase for the hydrolysis of bile acid conjugates. J Biol Chem 1984; 259: 15035-39.
57. Schmassmann A, Hofmann AF, Angellotti MA, Ton?Nu H?T, Schteingart CD, Clerici C, Rossi SS, Rothschild MA, Cohen BI. Stenger RJ, Mosbach EH: Prevention of ursodeoxycholate hepatotoxicity in the rabbit by conjugation with N?methyl amino acids. Hepatology 1990; 11: 989-996.
58. Schoelmerich J, Becher M-S, Schmidt K, Schubert R, Dremer B, Feldhaus S, Gerok W.: Influence of hydroxylation and conjugation of bile salts on the membrane-dmaging properties studies on isolated hepatocytes and lipid membrane vesicles. Hepatology 1984; 4: 661-6.
59. Miyazaki K, Nakayama F, Koga A: Effect of chenodeoxycholic and ursodeoxycholic acids on isolated adult human hepatocytes. Dig Dis Sci 1984; 29: 1123-30.
60. Quist RG, Ton-Nu H-T, Lillienau J, Hofmann AF, Barrett KE. Activation of mast cells by bile acids. Gastroenterology 1991; 101: 446-56.
61. Schmassmann A, Angellotti MA, Ton?Nu HT, Schteingart CD, Marcus SN, Rossi SS, Hofmann AF: Transport, metabolism and effect of chronic feeding of cholylsarcosine, a conjugated bile acid resistant to deconjugation and dehydroxylation. Gastroenterology 1990; 98: 163?174
62. Lillienau J, Schteingart CD, Hofmann AF: Physicochemical and physiological properties of cholylsarcosine: a potential replacement detergent for bile acid deficiency states in the small intestine. J Clin Invest 1992; 89: 420-431.
63. Longmire-Cook SJ, Lillienau J, Kim YS, Schteingart CD, Danzinger RG, Esch O, Hofmann AF: Effect of replacement therapy with cholylsarcosine on fat malabsorption associated with severe bile acid malabsorption: studies in dogs with ileal resection. Dig Dis Sci 1992; 37: 1217-1227.
64. Schmassmann A, Fehr HF, Locher J, Lillienau J, Schteingart CD, Rossi SS, Hofmann AF: Cholylsarcosine, a new bile acid analogue: metabolism and effect on biliary secretion in humans. Gastroenterology 1993; 104: 1171-81
65. Ricci P, Hofmann AF, Hagey LR, Jorgensen RA, Lindor KD: Adjuvant cholyl sarcosine during ursodeoxycholic acid treatment of primary biliary cirrhosis. Dig Dis Sci 1998;43: 1292-95.
66. Black RB, Hole D, Rhodes J: Bile damage to the gastric mucosal barrier: the influence of pH and bile acid concentration. Gastroenterology 1971; 61: 178-84.
67. Popovic OS, Jojic N, Necic D. Cholylsarcosine for bile salt deficiency caused by ileal resection. Dig Dis Sci 1999; 44: 1931-2.
68. Popovic O, Jojic N, Nackawic D, Milutinovic-Duric S, Dordevic D: Cholylsarcosine use for bile acid replacement in massive ileal resection: the effects on steatorrhea and diarrhea and the role of drug formulation. Arch Gastroenterohepatol 1998; 17: 2-18.
69. Gruy-Kapral C, Little KH, Fordtran JS, Hagey LR, Hofmann AF: Conjugated bile acid replacement therapy for short bowel syndrome: a comparison of cholylsarcosine and a natural bile acid mixture. Gastroenterology 1999; 116: 15-21.
70. Jeppesen PB, Mortensen PB: Colonic digestion and absorption of energy from carbohydrates and medium-chain fatty fat in small bowel failure. J Parenteral Enteral Nutr 1999; 23: S101-5.
71. Jeppesen PB, Mortensen PB:Intestinal failure defined by measurements of intestinal energy and wet weight absorption. Gut ((n press).
72. Heydorn S, Jeppesen PB, Mortensen PB: Bile acid replacement therapy with cholylsarcosine for short-bowel syndrome. Scand J Gastroenterol 1999; 34: 818-23.
73. Weinand I, Hofmann AF, Jordan A, Caspary FW, Stein J: Cholylsarcosine use for bile acid replacement in short bowel syndrome. Gastroenterology 1999; 116: A102 (abstract)
74. Ammon HV, Phillips SF: Inhibition of colonic water and electrolyte absorption by fatty acids in man. Gastroenterology 1973; 65: 744-9.
75. Messing P, Beau P, Boutron-Rualt MC, Rambaud J-C, Matuchansky C. Long-term survival and parenteral nutrition dependence in adult patients with the short bowel syndrome. Gastroenterology 1999: 117: 1043-50.
76. Gu J-J, Hofmann AF, Ton-Nu H-T, Schteingart CD, Mysels KJ: Solubility of calcium salts of unconjugated and conjugated natural bile acids. J Lipid Res 1992; 33: 35-46.
77. Hofmann AF, Mysels KJ: Bile acid solubility and precipitation in vitro and in vivo: the role of conjugation, pH, and Ca2+ ions. J Lipid Res 1992; 33: 617-26.
78. Heuman DM, Vlahcevic ZR, Pandak WM, Hylemon PB, Kim YS, Lilleanau J, Hofmann AF: Effect of cholylsarcosine on hepatic dholesterol and bile acid synthesis and bile secretion in rats. Gastroenterology 1992; 103: 1641-8.