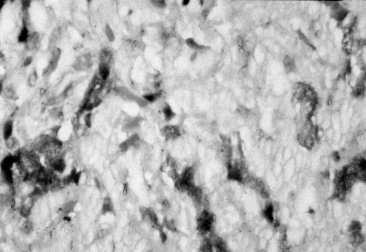
Figure 1.
The Liver In Systemic Amyloidosis
Jetra U Sistemskoj Amiloidozi
(accepted September 29th¸ 1999 )
Gradimir Golubovic, Ratko Tomaevic, 1Steva Pljea, Lidija Burg,2 Dejan Opric, Alja Vlahovic
Department of Gastroenterology, Service of Internal Medicine, Clinical Hospital Center Zemun, 1Department of Nephrology, Service of Internal Medicine, Clinical Hospital Center Zemun,Belgrade, 2 Institute of Pathology of Belgrade School of Medicine, Belgrade.
Address correspondence to:
Professor Dr Gradimir Golubovic
Department of Gastroenterology
Clinical Hospital Center Zemun
Vukova 9 11080 Beograd, Yugoslavia
Tel.( 381 11 ) 106 106
Systemic amyloidosis and liver Golubovic G. et al.
SUMMARY
We report the case of two patients with primary systemic amyloidosis. Beside the other organs
Involvement e.g. congestive heart failure, nephrotic syndrome¸ and skin changes both patients
had firm hepatomegaly, which required biopsy. Liver histology demonstrated perisinusoidal
amyloid deposits. In one patient primary amyloidosis was confirmed by serum monoclonal IgG
lambda light chains. After a 3-month treatment with corticosteroids both patients improved
clinically and laboratory.
Key words: Systemic amyloidosis, liver, heart¸ kidney.
SAZETAK
Prikazuje se slucaj dvoje pacijenata sa primarnom amiloidozom. Pored zahvacenosti vie organa: kongestivne srcane slabosti¸ nefrotskog sindroma¸ i promena po koi¸ oba bolesnika su imala uvecanu i cvrstu jetru to je zahtevalo biopsiju ovoga organa. Histologija jetre je pokazala
perisinusoidalne depozite amiloida. U jednog pacijenta primarna amiloidoza je dokazana prisustvom monoklonskih IgG lambda lakih lanaca u serumu. Posle tromesecnog lecenja sa
glukokortikoidima oba pacijenta su se klinicki i laboratorijski poboljali.
Kljucne reci: sistemska amiloidoza, jetra, srce¸bubreg.
INTRODUCTION
Amyloidosis is the colective name given to a group of different disease conditions whose common feature is the extracellular deposition of insoluble amyloid ( 1 ).This is usually an acquired condition although there are several hereditary amyloid syndromes ( 1 ). Deposits are sometimes
localised to one organ or may be systemic when amyloid is found in several visceral systems ( 2 ). The systemic disease is usually fatal and the clinical findings are due to the deposition of amyloid in vital organs¸ where it causes organ malfunction because of its excessive presence in the tissue ( 1¸2 ).
The amyloidoses are classified according to the type of deposited amyloid ( 1¸3¸4¸). Although a variety of types of amyloids have been described ( 12 in total )¸ the two major types¸ designated AL ( primary amyloid ) and AA ( secondary amyloid ) accounts for about 90% of cases ( 1¸2¸3¸4 ) .
In patients with primary ( AL ) amyloidosis the amyloid frequently¸ but not ultimately consists kappa or lambda immunoglobulin light chains produced by a monoclonal population of plasma cells ( 1¸3¸5 ). This is systemic¸ multi - organ disease variant which occurs without pre-existing disease ( 1¸2 ).
In secondary amyloidoses ( AA )¸ the amyloid is mainly derived from serum amyloid A ( SAP ) in response to chronic infections or inflammatory processes such as tuberculosis osteomyelitis¸ rheumatoid arthritis and lymphoma¸ as well as in amylodisis associated with familial Mediterranean fever ( 4¸6 ).
Systemic amyloidosis often involves the liver¸ primarily in AL - amyloidosis ( 54% AL vs 18% AA ) ( 1¸2¸3¸6¸7¸8 ). AA amyloid predominantly affects walls of the blood vessels in the portal tract thus constituting " vascular pattern " ( 9¸10 ). AL amyloid additionally exhibits " sinusoidal pattern " of distribution. ( 9¸10 ). Liver amyloidosis usually manifests by marked hepatomegaly and elevated serum alkaline phosphatase with normal transaminases ( 1¸3¸6¸7¸11¸12 ). Although portal hypertension is a rare complication, it was documented in 20% of patients and cholestatic icterus in 5% ( 13¸14 ).
Here we report two patients with systemic amyloidosis involving several organs including liver.
CASE REPORTS
Case 1 A 38-year-old electrician was admitted to the hospital because of fatigue, dyspnoea¸ heart palpitation, central cyanosis¸ ankle oedema¸ abdominal distension and jaundice. Blood pressure was normal. He was clinically found to have firm massive hepatomegaly¸ slightly enlarged spleen¸ and free peritoneal fluid. Cutaneous changes were present in both inguinal regions. They were maculopapulous eruptions.
Laboratory findings were as follow : ESR 105 mm / 1h, normal blood count¸ increased conjugated bilirubin ( 90 mmol/L ), hypoproteinemia ( 43g/L ), hypoalbuminemia ( 20 g/L )¸ normal transaminases and serum electrolytes¸ increased GGT ( 68 U/L)¸ high serum alkaline phosphatase ( 1160 U/L ). BUN was 24 mmol/L serum creatinine 222 umol/L, proteinuria 6 g / day, SAAG was over 11 g/L ( 20 g / L ) corresponding to a transudate. Bacteriology and cytology of ascitic fluid was negative. The ECG was of low voltage without ST-changes.Echocardiography showed marked hypertrophy of the left ventricular wall and septum ( 1.6 cm ) with granular hyperechogenic structure characteristic of infiltrative cardiomyopathy. Oesophagogastroduodenoscopy and rectosigmoidoscopy were normal. Rectal mucosal histology was normal as well. Abdominal ultrasound examination showed large hypoechogenic liver with interpolated fibrous strips but without signs of cirrhosis. The spleen was also markedly enlarged. Both kidneys were increased in size¸ hypoechogenic with parenchymal oedema. Liver histology demonstrated a presence of large amount of amorphous pink material in the space of Disse with haematoxylin and eosin. This material stained green with Congo red and had birefringent fibrilar pattern by polarization microscopy. The liver cell trabeculae were narrowed due to compression. Serum protein electrophoresis demonstrated increased alpha-2 and beta - globulins¸ decreased albumin¸ and abnormal protein band behind beta - globulin fraction which differentiation with specific antibodies was negative; the same refers to urine where paraproteins were negative. Beside increased IgM¸ serum immunophoresis was normal. Bone marrow aspiration biopsy was normal. HBO antigen anti - HCV¸ and anti - HIV 1 and 2 antibodies were all negative
The patient was treated with diuretics, albumin infusions¸ corticosteroids ( methylprednisolone 40 - 80mg / 24h ) and cardiotonics. At discharge patient ¸ s clinical condition was improved: proteinuria decreased to 1.6 g / day, BUN 12 mmol / L ¸ serum creatinine 160 umol / L. Three months later , the patient continued to be clinically stabile: ascites was reduced¸ cardiovascular functions improved¸ the nephrotic syndrome indices persisted.
Case 2 A 67-years-old retired man was admitted because of fatigue, ankle oedema and jaundice. Arterial BP was 130/80 mmHg; heart rate 150 / min.. Liver was palpable 10 cm below the right costal margin. Moderate ascites and ankle oedema were present as well. Laboratory studies were as follow: ESR 55 mm/ 1h, RBC 3.3 x 109 / L, Hgb 108 g / L, AST 97 U /L, ALT 41 U / L, conjugated bilirubin 70 mmol / L, total serum proteins 53 g / L, albumin 27 g / L, and increased alkaline phosphatase 998 U / L. BUN varied from 15.3 mmol to 23.4 mmol / L; serum creatinine from 454 umol / L to 582 umol / L. 24h proteinuria was moderate: 1.2 g. Serum protein electrophoresis revealed: low albumin fraction 49%, normal alpha 1 - globulins¸ increased alpha 2- 11.6 %, beta- 13.4 % and gamma - globulins 21.3%. Beta-2 microglobulin was 3.9; serum and urinary osmolality were normal. Monoclonal protein IgG with lambda light chains was positive in the serum¸ but negative in the urine. Bone marrow examination was normal.Viral markers for HBV and HCV were negative as well as ATP and CEA. Immunoelectrophoresis revealed increased IgG 237 mg / dl only ( normal value < 173 ). Chest radiography demonstrated myopathic heart¸ bilateral pleural¸ and pericardial effusions ECG showed lower QS in V1 to V3 only. Echocardiography was characteristic for restrictive myocardiopathy. Left ventricle was not dilated, but had a signs of concentric hypertrophy and hypocontractility of the septum and ventricular wall. A specific diffuse refractivity with sparkling reflection possibly indicated cardiac amyloidosis was noticeable .Abdominal ultrasound showed enlarged hypoechogenic liver without focal changes, small amount of ascites, normal spleen and dilated portal vein. Oedematous hypoechogenic renal cortex without collecting system changes was found as well. Rectal mucosal biopsy demonstrated blood vessels changes, which were affected with amyloid. On the contrary histological examination of gingiva was negative. Liver biopsy revealed massive perisinusoidal amyloid deposits suggesting primary amyloidosis.
Patient was treated with diuretics, ACE inhibitors and corticosteroids (methyprednisolone 40 mg / 24h ). This led to clinical improvement although azotemia persisted. Three months later BUN was normal; restrictive myocardiopathy was compensated. There were no ascites, no peripheral oedema, but alkaline phosphatase remains elevated.
DISCUSSION
Amyloidosis is disorder or protein metabolism that leads to extracellular deposition of insoluble material which appears homogenous and amorphous when viewed by light microscope and birefringence ( read: refracting twice¸ splitting a ray of light in two ) with polarising microscope ( 1 ). Despite these relatively uniform optical characteristics amyloid deposits are produced by variety of diseases of diverse etiology ( 1 ). On the contrary to localised amyloidosis or tumour - forming amyloidosis¸ systemic disease affects several organs ( 1¸4 ).
Clinical classification of systemic amyloidosis is based on the presence or absence of accompanied diseases and the multi - organ distribution of the amyloid deposits ( 1 ). Secondary amyloidosis is associated with variety of underlying chronic inflammatory processes. It is characterised with typical distribution pattern in liver¸ spleen¸ kidneys¸ and adrenals ( 1¸ ). In primary amyloidosis no underlying cause could be indentified. In this variant and in amyloidosis complicating multiple myeloma there is an atypical tissue distribution pattern involving heart¸ lymph nodes¸ nerves¸ muscle¸ tongue¸skin and gut ( 1¸4 ).
Amyloid is insoluble material made by three components ( 1¸3¸4¸ ). The first is the protein present in all chemical variants of amyloid called amyloid P ( AP ) which is syntetised by liver. The circulating form ( SAP ) consists two AP pentamers. It binds the fibrilar amyloid component protecting the latter of proteolysis because of its protease inhibiting capacity ( 1¸3 ). The second component is so called fibrilar protein, which varies in diferent forms of the disease ( 1¸3 ). In multiple myeloma these are immunoglobulin light chains kappa and gamma ( 5 ). The third amyloid component linked covalently with fibrilar protein is tissue glycosaminoglycanes. These are heparin sulphate and dermatan suphate, which gives to the amyloid anti - clotting activity ( 1¸3 ). There is classification systems based on the nature of the fibrilar protein component.
Systemic amyloidosis usually presents with fatigue¸ weight loss¸ oedema¸ paresthesia¸ purpura¸
bone pain¸ postural hypotension¸ biting of tongue¸ gastrointestinal bleeding¸ and diarrhoea thus
indicating amyloid involvement of different organs¸ e.g. heart failure¸ autonomic neuropathy¸
macroglossia¸ gastrointestinal mucosal amyloid deposition etc ( 1¸2¸3 ).
Systemic amyloidosis oftenly involves the liver ( 17% to 98% in different series ) ( 1¸3¸6¸7¸11¸12 ). Liver is enlarged in 20% to 40% of patients. Normal transminases¸ elevated alkaline phsphatase¸ abnormal PT time¸ and hypoalbuminemia are common laboratory abnormalities. Hyperbilirubinemia is very rare except as preterminal event ( 1¸ 14 ). However there is poor correlation between liver function tests abnormalities and degree of hepatic involvement ( 1¸3¸6¸7¸15 ). Gross hepatomegaly¸ hard liver in consistency¸ pain and tenderness on palpation in the absence of other signs of primary liver disease sometimes may prevail ( 1¸3¸6¸7¸15 ). Nephrotic syndrome may coexist with liver involvement thus leading to hypoalbuminemia and hypercholesterolemia ( 16 ).
Diagnosis of amyloidosis requires histologic evidence of amyloid deposition because there is no laboratory test, which is specific for this syndrome ( 17 ). Immunohistochemistry using specific antisera is necessary to determine the true nature of proteins, which form amyoid fibrils. The least invasive diagnostic essay is rectal ( and subcutaneous fat ) biopsy which is diagnostic in up to 80% of cases of systemic amyloidosis as renal biopsy as well ( 1¸3 ). Therefore it is not necessary to verify that a patient with with already confirmed systemic amyloidosis and hepatomegaly has liver amyloid disease which rarely causes significant morbidity ( 1 ). Liver biopsy does carry increased risk of bleeding. But if the diagnosis of amyloidosis is suspected but unconfirmed¸ the liver biopsy is indicated providing that platelet count and clotting abnormalities are corrected ( 1¸6 ). In the liver¸ amyloid is deposited in form of amorphous¸ hyaline material in the walls of arterioles and in the space of Disse predominantly ( 6 ). Therefore three basic deposition peterns have been described: space of Disse and sinusoidal¸ intralobular type ( more frequent in secondary AA amyloidosis )¸ vascular and periportal¸ and mixed type ( more frequent in primary AL amyoidosis ) ( 1¸17 ). Amyloid deposits distort and compress the normal hepatocyte plates thus leaving little of normal hepatic parenchyma..
Our cases further support the very variable expression of systemic amyloidosis and diagnostic difficulties ( 19 ). Clinical signs and laboratory indices of hart failure, nephrotic syndrome and firm haptomegaly possibly indicating cirrhosis and manifesting with dyspnea¸ cyanosis¸ ascites and peripherxic oedema were present in both cases. In addition splenomegaly and dilated portal ( by ultrasound ) suggested portal hypertension. Both patients were icteric what further masqueraded amyloidosis clinically¸ because in primary amyloidosis cholestasis is very rare.Normal transaminases¸ high alkaline phosphatase¸ and abnormal clotting in both patients with heart failure¸ nephrotic syndrome¸ ascites and negative rectal biopsy in one case were difficult to interpret at first. Typical echocardiographic features of myocardial amyloid deposits¸ and Doppler ultasonography were crucial in determining the origin of ascites in our patients. These findings coupled with clinical and laboratory parameters of nephrotic syndrome further explained ascites and directed further diagnostic procedures¸ e.g.liver biopsy. Therefore this is to confirm that nephrotic syndrome is usually equally present in systemic AL and AA amyloidosis ( 53% vs 47% ) ( 16 ). In the first patient urinary paraproteins were not found in spite of serum lambda light chain paraproteins positivity; in the second case the other pathologic proteins in beta fraction was found but not identified. In order to find the underlying pathological process extensive clinical and laboratory investigations were made and were negative in both cases.
In our patients liver histology revealed discrete perisinusoidal and portal arteriolar amyloid deposits. The findings were similar in both patients. Bilateral amyloid clusters were more dominant in sinusoids than in blood vessels. Hepatocytes were slightly atrophic and biliary stasis discrete. This pathological finding favored more primary amyloidosis what was in accordance with previous reports ( 17¸21 ). Hepatic amyloidosis is confirmed by positivity of paraproteins IgG of lambda class thus enabling us to make the diagnosis of AL - type amyloidosis in the first case, which had normal rectal biopsy and negative paraproteins in serum and urine.
There is no specific treatment for AL-type amyloidosis; however, corticosteroids, colchicine and melphalan (20) can prolong the survival time. There is no difference in survival of patients treated with colchicine and those treated with corticoids and melphalan ( 19 ). The mean survival time in AL amyloidosis is about 12 months after the diagnosis, and 9 months if portal hypertension is present. It was found that the main risk of early death was congestive heart failure ( 1¸2¸3 ). In patients with marked cholestasis and mean survival time is only 3 months. In our patients we demonstrated positive short - term effect of corticosteroids on myocardial functions and nephrotic syndrome.
In conclusion we presented two patients with systemic primary amyloidosis involving different organs. Both were mildly cholestatic and demonstrated firm non- - cirrhotic hepatomegaly. This necessitated liver biopsy which the most important for the diagnosis. Corticosteroids had positive initial effect on disease process.
REFERENCES
1.McAdam KPWJ. Amyloidoses. Mc Intyre N¸ Benhamou JP¸ Bircher J¸ Rizzeto M¸ Rodes J¸ eds. In: Oxford Textbook of Clinical Hepatology¸ 1st ed. Oxford : Oxford Medical Publications¸ 1992; 779 - 87
2.Kyle RA, Greip PR, Garton JP et al. Primary systemic amyloidosis: clinical and laboratory features in 474 cases. Semin Haematol 1995; 32:45.
3.Thiele DL¸ Eigenbrodt EH. Hepatic manifestations of systemic disease. Feldman M¸ Scharschmidt BF¸ Sleisenger M¸ eds. In: Sleisenger and Fordtran ¸ s Gastrointestinal and Liver Disease¸ 6th ed. Philadelphia : WB Saunders¸ 1998; 1388 - 1408.
4.Cohen AS, Conors LH. The pathogenesis and biochemistry of amyloidosis. J Pathol 1987;151:1-5.
5.Faa G, Van Eyken P, De Vos R et al. Light chain deposition diseases of the liver associated with AL- type amyloidosis. J Hepatol 1991; 12:75-82.
6.Cohen AS, Skiner M. Amyloidosis of the liver. In: Schiff L, Schiff ER eds. Diseases of the 6th edition Philadelphia : JB Lippincott 1988; 1093-1108.
7. Sherlock Sh. Hepatic amyloidosis. In: Sherlock S¸ Dooley J¸ eds. Diseases of the liver and biliary system. 10th edition, Oxford : Blackwell¸ 1997; 442-445..
8.Lovrat LB, Presey MR, Madhoo S et al. The liver in systemic amyloidosis. Gut 1988; 42:727-734.
9.Loci I , Sumithan E. Morphological differences in the pattern of liver infiltration between AL and AA amyloidosis. Human Pathol 1988; 19: 732-..
10.Buck FS, Joss MN. Hepatic amyloidosis: morphological differences between systemic AT and AA-types. Hum Pathol 1991; 22: 904-907.
11.Iwata T, Hoshii Z, Kawano H et al. Hepatic 1.amyloidosis in Japan: histological and morphologic analysis based on amyloid proteins. Hum Pathol 1995;26:1148-1153.
12.Gerty MA, Kyle RA. Hepatic amyloidosis: Clinical appraisal in 77 patients Hepatology 1997; 25: 118-121.
13.Bion E, Brenard R, Pariente EA. Sinusoidal portal hypertension in hepatic amyloidosis. Gut 1991; 32:227-230.
14.Peters RA. Koukoulis G, Gimson A et al. Primary amyloidosis and severe intrahepatic cholestatic jaundice. Gut 1994; 35:1322-5.
15.Gertz MA, Kyle RA. Hepatic amyloidosis (AL): The natural history in 80 patients. Am J Med 1988; 95: 73-80.
16.Gregg JA, Herskovic T , Bartholonce IG. Ascites in systemic amyloidosis. Arch Intern Med 1965¸116 605 - 10.
17.Chopra S , Rubinow A, Koff Rs et al. Hepatic amyloidosis. A histological analysis of p rimary (AL) and secondary (AA) form, Am J Pathol 1984; 115: 186-193.
18.Gerty MA , Kyle RA . Hepatic amyloidosis: clinical appraisal in 77 patients. Hepatology 1997; 25 : 118-21.
19.Griepp P. Amyloidosis (AL). An approach to early diagnosis. Arch Intern Med. Med 1965; 116:605-10
20.Kyle RA, Griepp P, Garton JP, Gertz MA. Primary systemic amyloidosis. Comparison of Melphalan / Prednisone versus Colchicine. Am J Med 1985; 79: 708-16.
Figure 1.
Hepatic amyloidosis: note large amount of perisinusidal amorphous eosinophyl material which corresponds to amyloid ( 400 x )..
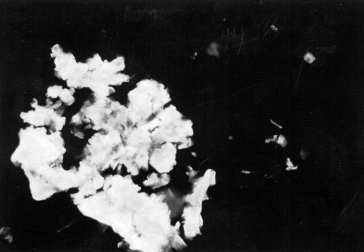
Figure 2.
Hepatic amyloidosis: amyloid deposits demonstrates positive fluoresscency ( Thioflavin, 100 x )