Gastroenterohepatoloska ikonografija
ARCH GASTROENTEROHEPATOLOGY 2001; 20 ( No 3 - 4 ):
1Mira Petrovic
2Dejan Opric
1Vojislav N. Perisic
1Dragana Kukobat
1University Children , s Hospital, Belgrade,
2Institute of Pathology, Faculty of Medicine, Belgrade.
Address correspondence to: Professor Dr Vojislav N. Perisic
University Children , s Hospital
Tirsova 10 St,
YU-11000 Belgrade, Serbia, Yugoslavia
E-mail: [email protected]
Coeliac mucosal topography changes by videoduodenoscopy with tissue
staining (methylene-blue)
Prikazivanje celijacnih promena topografije crevne sluznice videodudeonskopijom
sa tkivnom bojom ( metilensko-plavo)
( accepted December 19th, 2001 )
An eleven-year old boy with syndromic form of congenital intrahepatic biliary hypoplasia (Alagille syndrome) and portal hypertension developed chronic diarrhoea with steatorrhoea, abdominal bloating, meteorism, and weight loss. Spleen was enlarged. Haemoglobin level was 106, WBC 3.8, trombocyte 90. Previous endoscopic examinations demonstrated oesophageal varices of grade I. Signs or portal gastropathy were absent. Doppler ultrasonography of lieno-portal venous system demonstrated centripetal but significantly decreased portal blood flow velocity. Stool cultures for bacterial pathogens and faecal microscopy for ova of parasites were negative. IgA and IgG antigliadin antibodies serum concentrations were were high.
Duodenoscopy was performed on outpatient basis. Paediatric gastroduodenoscope was introduced below the main duodenal papilla in a blind manner without air insufflation. When duodenum was insufflated with the air, 4ml of 1% methylen-blue was spayed over the overlying mucosa and duodenoscopic images were recorded on videotape. This was followed by endoscopic duodenal mucosal biopsies, and procedure was completed.
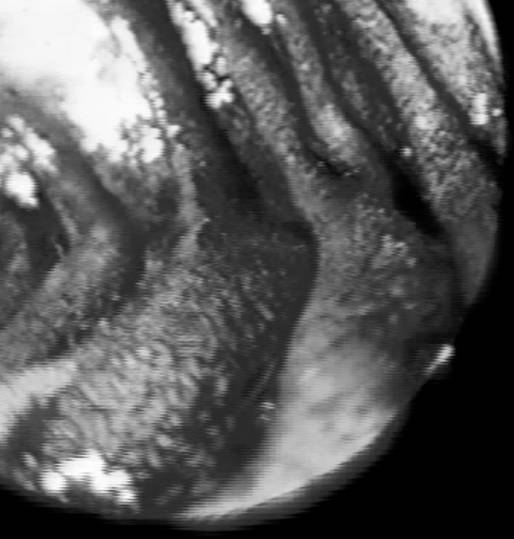
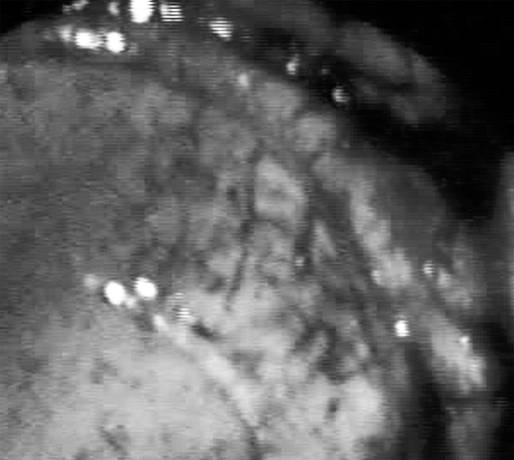
The taped videoduodenoscopy was analysed immediately after procedure and abnormal videoendoscopic markers were recorded. They were as follow:
immediate visualisation of underlying mucosal blood vessels after injection of very few drops of 1% methylen-blue
“ flat” mucosal surface with visible transversal mucosal clefts ( narrow,linear depressions): reticular pattern of mucosal surface
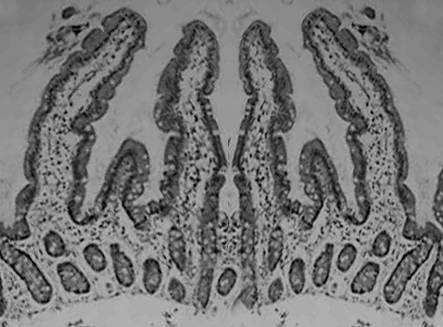
Histopathologal report of endoscopic duodenal mucosal biopsies was: total villous atrophy, dense limpho-plasmocytic infiltrate in the lamina propria, elongated crypts, increased mitoses on the bases of the crypts. FIGURE 1, 2.
The child was put on gluten-free diet. Follow-up examinations demonstrated amelioration of diarrhoea and weight gain. Laboratory signs of hypersplenism persisted.
Comment: There is increasing evidence that video-assisted endoscopy with contrast stain (1% methylen-blue) of duodenal mucosa allows to the endoscopist to assess the intestinal surface morphology of large areas of mucosa (1). This facilitate delineation of mucosal abnormalities in coeliac disease (CD), e.g. villous atrophy. The sensitivity and specificity of this method is exceeding 90% (1). To recognise endoscopic markers of CD particularly in adult patients with non-specific symptoms referred to upper GI endoscopy, videochromoendoscopy of the duodenal mucosa with contrast stain may be of relevance. These signs are as follow:
visualisation of underlying mucosal blood vessels ( because of disappearance of intestinal villous covering )
mosaic pattern of the mucosa: recognised as geometric reticular pattern
reduction of duodenal circular folds, their absence or critical diminution at maximum air insufflation
Videochromoendoscopy understands tissue staining during videoendoscopic procedures. In order to highlight subtle mucosal surface changes contrast stains are introduced within the gut lumen or permanent stains are injected (tattooing) in targeted mucosal changes (1,2,3).
The contrast stains currently used in come centers during videochromoendoscopy procedures are as follow:
1% Lugol , s solution: to stain glycogen containing non-keratinized squamous epithel (normal oesophageal mucosal lining) demarcating normal oesophageal epithelium from columnar, malignant epithelium, or dysplastic epithelium of Barrett , s epithelium.
1% Methylen-blue solution: is vital stain taken by absorptive intestinal epithelium. Initially, this stain is used to detect intestinal metaplasia in the stomach to possibly diagnose earlier gastric cancer or in surveillance purposes.
India ink tattooing suspected colonic dysplastic or premalignant lesions.
In summary, vital dye staning during endscopy may be of relevance in detecting mucosal changes, e.g. in coeliac disease in particular. This method has to be freely performed in significant proportion of dyspeptic patients, which may potentially suffer of coeliac disease. Mucosal vital dye staining during videochromoendoscopic procedures will definitely increase the number of diagnosed coeliac patients.
REFERENCES:
1.Niveloni S, Fiorini A, Dezi R et al. Usefulness of videoduodenoscopy and vital dye staining as indicators of mucosal atrophy of coeliac disease: assessment of interobserver agreement.
Gastrointest Endosc 1998; 47: 223-9.
2.Fennerty BM. Should chromoscopy be part of the proficient endoscopist , s armamentarium? Gastrointest Endopsc 1998; 47: 313-5.
3.Fennerty BM. Tissue staining. Gastrointest Endosc Clin N Am 1994; 4: 297-311.