ARCH GASTROENTEROHEPATOL 2001; 20 ( No 3- 4 ):
Institute of Digestive Diseases, Clinic for Gastroenterology and Hepatology, Clinical Centre of Serbia, Belgrade
Address correspondence to: Professor Dr Dragan Tomić
Hadži Ruvimova 5
11000 Beograd,
FAX: + 381 11 361 55 87
E-mail: [email protected]
Key words: Portal vein, blod velocity, portal hypertension.
Ključne reči: Portna vena, brzina toka krvi, portna hipertenzija.
Portal blood flow velocity in different conditions is important to study.
Decrease of bloow flow velocity is a reliable and sensitive diagnostic
criterium of the portal hypertension. We therefore performed a study to
evaluate whether drop of the portal blood flow velocity is a reliable diagnostic
criterium of portal hypertension. Another aim of this study was to explore
the possibility that the basic parameters of the portal blood flow can
be reliably measured without lieno-mesenteric-portal angiography.
The patient, s group included 60 cases, aged 53 on average, with portal hypertension diagnosed on the basis of the presence of esophageal varices (mainly of the 2nd and 3rd degree). The most common aetiology of portal hypertension was alcoholic liver cirrhosis (32 cases). Thirteen patients had posthepatitic cirrhosis. Four female patients had primary billiary cirrhosis, while 1 patient had primary sclerosing cholangitis. Regarding disease severity the majority were classified into the group B according to Child-Turcotte classification. A smaller number were group C according to the same classification.
The control group included 55 healthy individuals, aged 39 on average. This cases were referred for an ultrasonographic examination because of complaints that was proved to be of functional origin.
In order to detect oesophageal varices all patients suspected as having portal hypertension undergone upper GI endoscopy. Oesophageal varices were are classified into four grades, from 1 to 4 according to Paquet ( 2 ). The biggest number of patients with portal hypertension had varices of the grade 2 and 3.
In this study abdominal ultrasonography with pulsed and colour Doppler were used to study basic circulatory parameters of the portal system (3,4,5,6,7,8). Patients with varices and controls were examined with modern ultrasound units equipped with a pulsed and colour Doppler. The patients were examined at the Ultrasound Diagnostics Section of the Gastroenterological and Hepatological Clinic of the Clinical Centre of Serbia. The examination of the patients was made in the supine position, with an empty stomach, using a lot of transversal, longitudinal and oblique cross sections, and applying the so-called real time method. When the blood flow in the portal and splenic veins was visualised with colour Doppler and the pulsed Doppler, blood flow velocity was measured and calculated (9,10).
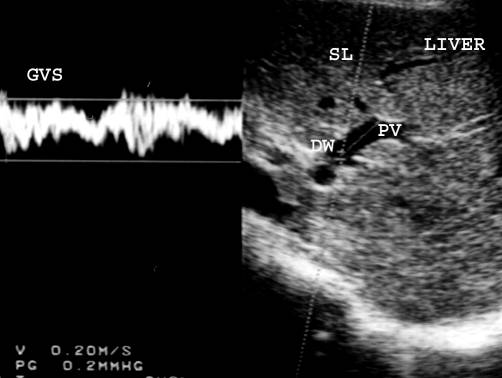
A classical ultrasound image is shown on the monitor where the segments of blood vessels the examiner is interested in, are coloured by the colour Doppler technique. By the pulsed Doppler technique, the examiner directs the narrow Doppler beam toward coloured segment of the blood vessel and outlines the scan line along which he can analyze the blood flow velocity. The analysis is made on the scan line which is marked with a special marker, a Doppler window. Its position in relation to the blood vessel is also determined by the examiner. Figure 1. An ideal conditions is when Doppler beam is parallel with the longitudinal axis of the blood vessel. In practice, the most common situation is when Doppler beam makes sharp angle of some degree in relation with the blood vessel axis. An angle of 60o is considered as upper limit when measurement is possible.
A graphic velocity spectrum is shown in a part of the monitor. These speed values are established in the area designated by the Doppler window. The time base is on the projected graph on x-axis while the ordinate y-axis is the velocity function. It is taken arbitrarily that the flow direction towards the probe be considered positive and it is brought over the positive part of the ordinate. The opposite direction (leading away from the probe) is considered as negative and it corresponds to the negative part of the ordinate on the graph, and it is shown under the x-axis.
The described method of examination makes possible to determine precisely the velocity or more precisely the distribution of the blood flow velocity values in the blood vessel at selected places. The numerical values of the blood flow velocity are shown automatically on the graph ordinate. The blood flow direction is determined in relation to the x-axis of the shown speed spectrum.
For all the values of the blood flow speed in the portal and splenic veins of the patients and the healthy controls we claclulated the arithemetic mean (X), standard deviation (SD), variation coefficient (V%), the maximum result (Max), the minimal result (Min) and the result range (R). The significance of the differences in the arithmetic mean of the blood flow speed with patients and healthy examinees was assessed by the calculation of the t-test. Starting from the values of both samples (N=60 and N=55), the difference in arithemetic mean values is statistically significant if the t-test value is equal or higher than the critical level of 1.98 (with the reliability of making a conclusion of 0.95).
The average blood flow velocity in the splenic vein in the patients with portal hypertension was 10.17 cm/s; in the control group 17.26 cm/s. This difference was statistically (t>t 0,001) as well. Table 3.
Several authors studied normal portal venous system haemodynamics by pulsed and colour Doppler technique. Zoli is his study of 82 patients, reported an average value of the portal vein blood flow velocity of 10.5 cm/s, and 16 cm/s in healthy individuals (17). According to Zironi, the average value of the portal vein blood flow velocity in healthy persons was 19.6 cm/s, while in patients with portal hypertension this was 13 cm/s (18). In this study we found an average value of the portal blood flow velocity in healthy controls 17.66 cm/s, range: 15-23 cm/s (15). Adding or deducting two standard deviations (which includes 95.5% of the examinees) this gives a range of 14.36-20.96 cm/s. In adition we found an average splenic vein blood flow velocity in healthy controls 17.26 cm/s, range: 15-23 cm/s. Adding or deducting two standard deviations (including 95,5% of the examinees) this gives a range of 13.46-21.06 cm/s.
Takayoshi, Saito, Shiraki, and Chawla demonstrated that in patients with portal hypertension of various aetiology, there is a considerable drop of the portal, splenic, and upper mesenteric vein blood flow velocity (16,19,20,21,22). According to this study and numerous other reports portal blood flow velocity decrease in the portal and splenic veins is a reliable ultrasonographic sign of portal hypertension (23,24).
In this study we demonstrated that average blood flow velocity in the portal vein in patients with portal hypertension was 9.38 cm/s, range: 6-13 cm/s. Figure 2. Adding and deducting two standard deviations (which includes 95.5% of the patients) this gives a range of 6.54-12.22 cm/s. As values of portal hypertensive patients were lower than in healthy examinees, it was important to define the cutt-off value of the blood flow velocity between patients and healthy controls. This was 12 cm/s. Consequently abnormal values of the portal blood flow velocities in portal hypertension is <12 cm/s More profound drop in the portal vein blood flow velocity is encountered in a cases with portal vein trombosis or in its main branches (29,30,31).
The flow pattern in the splenic vein in patients with portal hypertension has been previously studed. Using Doppler ultrasound, Barakat describes the intrasplenic venous flow direction in 176 adult patients with intrahepatic portal hypertension (35). In this study we found an average value of the blod flow velocity in the splenic vein in portal hypertension is 10.17 cm/s, range: 7-12 cm/s. Figure 3. When two standard deviations are added and deducted (which includes 95.5% of the patients sample group), this give a range 7.61-12.3 cm/s. The upper reference value is 12 cm/s, which means that all higher values are normal, and lower < 12 cm/s indicate portal hypertension.
Gastric mucosal blood in portal gastropathy manifested with GI bleeding is studied by several authors as well (25,26). Iwao demonstrated by laser Doppler technique very slow, slugish gastric mucosal blood flow velocity in patients with portal hypertension and hypertensive gastropathy (27,28).
In portal hypertension, portal blood flow velocity measurements may predict the risk of variceal bleeding. It is demonstrated by echo-Doppler flowmetry that in liver cirrhosis there is an insiginficant rise of postprandial portal blood flow. Postprandial rise of portal flow velocity is inversely related to the severity of portal hypertension in liver cirrhosis, and this appears to be valuable indicator of an increased risk of variceal bleeding (32). In Cioni's study it was shown that variations in portal vein Doppler sonographic parameters induced by administration of beta-blocker may predict long-term effects of these drugs in the prevention of a first episode of variceal bleeding (33). In addition, significantly lower portal flow velocity was observed in patients of fulminant hepatic failure with ascites compared with those without ascites (34).
The usefulness of color Doppler sonography in the detection of spontaneous portosystemic shunts and abnormal blood flow direction in the portal vein in patients with cirrhosis, were evaluated also. Portosystemic shunts and the direction and velocity of portal venous flow are important features in the sonographic diagnosis of portal hypertension (36).
This tehnique can be applied for arterial flow velocity measurement
too. Kito, prospectively measured the flow velocity and resistive index
of the common, right, and left hepatic arteries, using Doppler sonography,
in 21 patients who underwent embolization of the right portal vein. Portal
vein embolization induces an increase in hepatic arterial blood flow velocity
in the embolized hepatic segments, resulting from an increase in common
hepatic arterial flow. This observation may be explained by the simple
mechanical effect of interposing a slower flowing stream (portal flow)
in the path of a faster flowing stream (arterial flow)(37).
Using color Doppler and pulsed Doppler ultrasound, blood flow changes inside normally functioning transjugular intrahepatic portosystemic shunts (TIPS) can be evaluated. A velocity gradient between the portal and the venous side of a TIPS is a normal finding caused by branches of the portal and hepatic vein joining the TIPS from the side and it is characteristic of a normally functioning TIPS (38).
In conclusion, pulsed and colour Doppler technique are an important tool for qantitative measurements and assessment of hemodynamic parameters of the portal circulation in varienty of contidions, especially portal hypertension. The colour and pulsed Doppler method is of comparable sensitivity and preciseness with other invasive methods in assessing patients with suspected portal hypertansion. Direct visualisation of the blood flow and their parameters measurements considerably shortens the examination time (39,40).
REFERENCES:
1. Johnson LS, Kinnear DG, Brown RA, Mulder DS. “Downhill”
esophageal varices. A rare cause of upper gastrointestinal blooding. Arch
Surg 1978; 113: 1463-64.
2. Paquet KJ, Denck H, Zockler CE. Die Oesophagus-varizen-blutung. Bad Oeyen-Hausen: TM-Verlag 1984; 19-23.
3. Silva G, Fluxa F, Bresky G et al. Splanchnic and systemic hemodynamics
in early abstinence and after ethanol administration in non-cirrhotic alchoholic
patients. J Hepatol 1994; 20: 494-9.
4. Sabba C, Ferraioli G, Buonamico P et al. Echo Doppler evaluation
of acute flow changes in portal hypertensive patients: flow velocity as
a reliable parameter. J Hepatol 1992; 15: 356-60.
5. Zweibel WJ, Mountford RA, Halliwel MJ, Wells PN. Splanchnic blood flow in patients with cirrhosis and portal hypertension: investigation with duplex Doppler US. Radiology 1995; 194: 807-12.
6. D’Alimonte P, Cioni G, Cristani A, Ferrari A, Ventura E, Romagnoli R. Duplex Doppler ultrasonography in the assessment of portal hypertension. Utility of the measurement of maximum portal flow velocity. Eur J Radiol 1993; 17: 126-9.
7. Mito M, Sano F, Kasai S, Tamaki A, Kawamura A. Study on the hepatic
circulation in liver diseases by the ultrasonic Doppler method. Gastroenterol
Jap 1983; 8: 154-6.
8. Iwanaga T, Koyanagi N, Sugimachi K. Validity of ultrasonic duplex
system for measurement of the portal blood flow in patients with liver
diseases. Jap J Surg 1987; 17: 58-9.
9. Klews PM. Physics and technology of color duplex sonography. In:
Wolf KJ, Fobbe F. Color duplex sonography. New York: Thieme Medical Publishers,
1995: 245-94.
10. Grant EG, Schiller VL, Millener P et all. Color doppler imaging
of the hepatic vasculature. AMR 1992; 159: 943-50.
11. Lebrec D. Methods to evaluate portal hypertension. Gastroenterol
Clin North Am 1992; 21: 41-59.
12. Lomas DJ, Britton PD, Summerton CB, Seymour CA. Duplex Doppler
measurements of the portal vein in portal hypertension. Clin Radiol 1993;
48: 311-5.
13. Iwao T, Toynaga A, Oho K. Value of Doppler ultrasound parameters of portal vein and hepatic artery in the diagnosis of cirrhosis and portal hypertension. Am J Gastroenterol 1997; 92: 1012-7
14. Furuse J, Matsutani S, Saisho H, Ohto M. Hemodynamics of intrahepatic
portal vein studied in haelthy subjects and liver cirrhosis by pulsed Doppler
method. Nippon Shokakibyo Gakkai Zasshi 1992; 89: 1341-8.
15: Rehrer NJ, Smets A, Reynaert H, Goes E, De Meirleir K. Effect
of exercise on portal vein blood flow in man. Med Sci Sports Exerc 2001;
33: 1533-7
16: Piscaglia F, Donati G, Serra C, et al. Value of splanchnic Doppler ultrasound in the diagnosis of portal hypertension. Ultrasound Med Biol 2001; 27:893-9
17. Zoli M, Marchesini G, Cordiani MR, et al. Echo-Doppler measurement
of splanchnic blood flow in control and cirrhotic subjects. J Clin Ultrasound
1986; 14: 429-35.
18. Zironi G, Gaiani S, Fenyves D, Rigamonti A, Bolondi L, Barbara
l. Velue of measurement of mean portal flow velocity by Doppler flowmetry
in the diagnosis of portal hypertension. J Hepatol 1992; 16: 298-303.
19. Tanabe T, Tobe K, Koide N, et al. Blood flow dynamics in the
portal venous system in the liver diseases studied by the ultrasonic pulsed
Doppler method. Acta Hepatologica Japonica 1985; 26: 65-73.
20. Saito M, Erabayashi H, Wada K, et al. Ultrasonic measurement
of portal and splenic venous flow and their velocities in normal subjects
and patients with chronic liver disease. Acta Hepatologica Japonica 1984;
25: 1281-87.
21. Shiraci S, Tsucada K, Ozeki N, et al. Measurement of portal blood
flow by an ultrasonic duplex system composed of a pulsed Doppler flowmeter
and a linear-type real time B mode electroscanner. Gastroenterol Jap 1988;
23: 37-43.
22: Chawla Y, Sreedharan A, Dhiman RK, Jain S, Suri S. Portal hemodynamics
in fulminant hepatic failure as assessed by duplex Doppler ultrasonography.
Dig Dis Sci 2001; 46: 504-8
23: Yin XY, Lu MD, Huang JF, Xie XY, Liang LJ. Color Doppler velocity
profile assessment of portal hemodynamics in cirrhotic patients with portal
hypertension: correlation with esophageal variceal bleeding. J Clin Ultrasound
2001; 29:7-13
24: Erdozain Sosa JC, Martin Hervas C, Moreno Blanco MA, et al. Color
duplex Doppler ultrasonography in the evaluation of the risk of esophageal
varices bleeding in cirrhotic patients. Gastroenterol Hepatol 2000; 23:466-9
25: Kamath PS, Lacerda M, Ahlquist DA, McKusick MA, Andrews JC, Nagorney
DA. Gastric mucosal responses to intrahepatic portosystemic shunting in
patients with cirrhosis. Gastroenterology 2000; 118:905-11
26: Masuko E, Homma H, Ohta H, Nojiri S, Koyama R, Niitsu Y. Rheologic
analysis of gastric mucosal hemodynamics in patients with cirrhosis. Gastrointest
Endosc 1999; 49:371-9
27. Iwao T, Toyonaga A, Ikegami M, et al. Reduced gastric mucosal
blood flow in patients with portal hypertensive gastropathy. Hepatology
1993; 18: 36-40
28: Gupta R, Sawant P, Parameshwar RV, Lele VR, Kulhalli PM, Mahajani
SS. Gastric mucosal blood flow and hepatic perfusion index in patients
with portal hypertensive gastropathy. J Gastroenterol Hepatol 1998; 13:921-6
29: Palazzo L, Hochain P, Helmer C, et al. Biliary varices on endoscopic
ultrasonography: clinical presentation and outcome. Endoscopy
2000; 32: 520-4
30: Morales Perez J, Olloqui Martin E, Alcazar Iribarren M, et al.Collateral biliary circulation in portal hypertension syndrome. Rev Esp Enferm Dig 1999; 91: 759-68
31: Malkan GH, Bhatia SJ, Bashir K, et al. Cholangiopathy associated with portal hypertension: diagnostic evaluation and clinical implications. Gastrointest Endosc 1999; 49:344-8
32: Ludwig D, Schwarting K, Korbel CM, Bruning A, Schiefer B, Stange
EF. The postprandial portal flow is related to the severity of portal hypertension
and liver cirrhosis. J Hepatol 1998; 28:631-8
33: Cioni G, Turrini F, Tincani E, et al. Prevention of a first episode
of variceal bleeding: role of duplex Doppler sonographic measurement of
the acute response to beta-blockers. J Ultrasound Med 1999; 18: 633-8
34: Chawla Y, Sreedharan A, Dhiman RK, Jain S, Suri S. Portal hemodynamics
in fulminant hepatic failure as assessed by duplex Doppler ultrasonography.
Dig Dis Sci 2001; 46: 504-8
35: Barakat M, Hassan A, Soliman A, Nafeh M. Intrasplenic venous
flow patterns demonstrated by Doppler ultrasound in patients with portal
hypertension. Br J Radiol 1998; 71: 384-7
36: von Herbay A, Frieling T, Haussinger D.J. Color Doppler sonographic
evaluation of spontaneous portosystemic shunts and inversion of portal
venous flow in patients with cirrhosis. Clin Ultrasound 2000; 28: 332-9
37: Kito Y, Nagino M, Nimura Y. Doppler sonography of hepatic arterial
blood flow velocity after percutaneous transhepatic portal vein embolization.
AJR Am J Roentgenol 2001; 176:909-12
38: Bodner G, Peer S, Fries D, Dessl A, Jaschke W. Color and pulsed
Doppler ultrasound findings in normally functioning transjugular intrahepatic
portosystemic shunts. Eur J Ultrasound 2000; 12:131-6
39. Mostbeck G, Mallek R, Gebauer A, Tscholakoff D. Duplex ultrasound
and color coded Doppler ultrasound of visceral blood vessels in abdominal
diseases. Wien Klin Wochenschr 1992; 104: 227-33.
40. Calliada F, Bergonzi M, Passamonti C, et al. Portal hypertension
of hepatic origin: A qualitative assessment by color and echo Doppler US.
Radiol Med 1990; 79: 339-45.
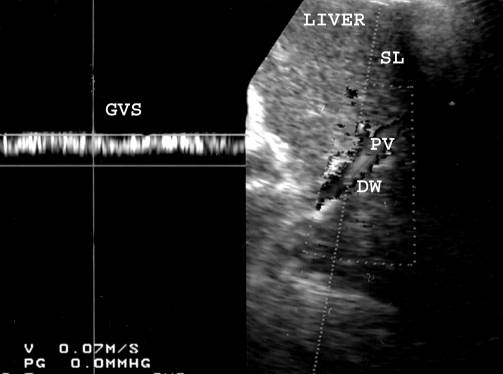
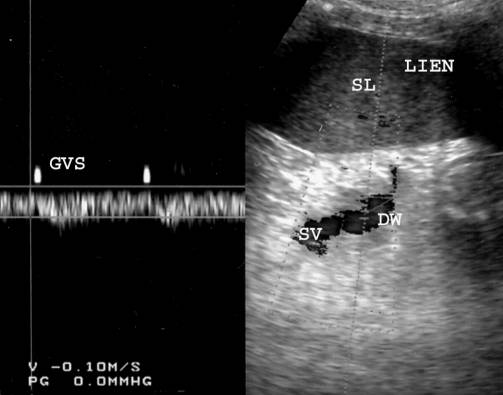
Table 1. Portal and splenic vein blood velocity in patients with portal hypertension
|
variable |
statistic
parameter |
|||||
X |
SD |
V% |
Max |
Min |
R |
|
|
Portal vein blood
velocity (cm/s) |
17,66 |
1,65 |
9,33 |
23,00 |
15,00 |
8,00 |
|
Splenic vein blood velocity (cm/s) |
17,26 |
1,90 |
11,00 |
23,00 |
15,00 |
8,00 |
Table 2. Portal and splenic vein blood velocity in healthy examinees
|
variable |
statistic
parameter |
|||||
X
|
SD
|
V%
|
Max
|
Min
|
R
|
|
|
Portal vein blood
velocity (cm/s) |
9,38 |
1,42 |
15,08 |
13,00 |
6,00 |
7,00 |
|
Splenic vein blood velocity (cm/s) |
10,17 |
1,28 |
12,57 |
12,00 |
7,00 |
5,00 |
Table 3. The significance of the differences in the arithmetic mean of the blood flow velocity with patients and control group
|
variable |
sample of patients |
control group sample |
t - test |
|||
|
X |
SD |
X |
SD |
t |
significance |
|
|
Portal vein velocity (cm/s) |
9,38 |
1,42 |
17,66 |
1,65 |
-28,95 |
t>t 0,001 |
|
Splenic vein velocity (cm/s) |
10,17 |
1,28 |
17,26 |
1,90 |
-23,28 |
t> 0,001 |