Alimentary tract and pancreas
Alimentarni trakt i pankreas
ARCH GASTROENTEROHEPATOL 2001; 20 ( No 3 – 4 ):
The role of SMS 201-995 as an experimental model in the intestinal ischemia-revascularisation
syndrome
Uloga SMS 201-995 na sindrom intestinalne ishemije-reperfuzije na eksperimentalnom
modelu
( accepted November 20th, 2001 )
1Fernando Fuertes- Guiró, 2Joan Viñas
Salas, 3Corrado d’Urbano
1International University of Catalonia, Barcelona, Spain,
2 Lleida Medical School. University of Lleida. Spain,
3 Department of Emergency Surgery, Provincial General
Hospital
of Milan, Milan, Italy.
Address correspondence to: Professor Fernando Fuertes-Guiró,
MD, PhD, PhD ( Eur )
International University of Catalonia
Calle Gomera s/n
E-08190
Sant Cugat del Vallés
Barcelona, Spain
FAX: +34 93 5042001
E-mail: [email protected]
ABSTRACT
AIMS: The main purpose of this research is to verify whether
the SMS 201-995 as the only therapeutical option, and using a research
protocol, has beneficial effects on the ischemia-revascularization syndrome.
MATERIAL AND METHODS: Sixty four male Wistar rats (32 for the
control group and 32 for the treated group) were randomized in four studies:
1. Biochemical study (36 hours of observation), obtaining preoperative
and postoperative quantitative data (Na, K, Cl, and bicarbonate intestinal
serum content); 2. Histological study: a) microscope, using 4 stains and
a score for the evaluation of the lesions; b) ultrastructurally with scanning
electron microscope, observation of objective variations on the surface
of villi; 3. Survival parenteral hydration (0.25 mL/100 gr. weight of Ringer
lactate and 0.1% of albumine) with yugular cannula, testing the Pi, the
BUN and the total survival on constant periods of time; 4. Survival
without hydration, observing only the total survival. The SMS 201-995 dose
was 10 ug/100gr./8h, subcutaneously.
RESULTS: The treated animal group maintained serum levels of
Na, K, Cl and bicarbonate closer to the basal levels than the control groups,
being the Na, K, Cl and bicarbonate significantly different. The 4 ions
concentration and content of the guts and the volume of intestinal content
were significantly lower on the treatment group. The histological
lesions of the guts was also better among the treatment group. The treated
group- with or without hydration- increased the survival level. The quantitative
grade of variation and the velocity of variation of the BUN and the Pi
in blood was significantly lower among the treatment group.
CONCLUSIONS: The SMS 201-995 or octreotide, as the only
pharmacological option during the revascularization period on a controlled
ischemia-revascularization syndrome, reduces the intestinal liquid retention,
mantains the absorption- secretion intestinal process ( which has
a positive effect in the intravascular space), and reduces the severity
of the lesions in the gut. The cytoprotective effect, the protection
on a catabolic stress situation and the capacity to maintain a reasonableb
level of volemia should permit to prolonge the animal’s survival.
Key words: octreotide, ischemia-revascularization, gut, survival,
intestinal absorption- secretion.
SAZETAK
CILJEVI: Glavni cilj ispitivanja je da se utvrdji da li SMS 201-995
kao jedino terapijsko sredstvo u istrazivackom postutku ima povoljan efekat
na sindrom ishemije-revaskularzacije.
MATERIJAL I METODE: 64 Wistar miseva ( 32 kontrolna grupa, 32 lecena
grupa ) su bili su metodom slucajnog izbora ukljuceni u 4 ispitivanja:
1.Biohemijska studija ( posmatranje tokom 36h ) koja je podrazumevala pre-
i postoperativno pracenje Na,K,Cl,HCO3 u serumu iz creva; 2.Histoloska
studija: a)mikroskopski pregled koji je ukljucivao 4 vrste bojenja i stepenovanje
crevnih ostecenja; b)ultrastukturno ispitivanje “scanning”
elektronskim mikroskopom u cilju utvrdjivanje promena crevnih resica; 3.Tokom
primene parenteralne hidracije preko jugularne kanule u cilju prezivljavanja
( 0.25 ml/100gr tezine Ringer lactata and 0.1% albumina
) mereni su P i azotne materije ( urea ) i duzina prezivljavanja u definisanom
vremenskom periodu; 4. Merenje prezivljavanja bez hidracije. Doza SMS 201-995
je bila 10 ug/100gr/8h potkozno.
REZULTATI: U lecenih zivotinja odrzavani serumski nivoi Na,K,Cl,
HCO3 su bili blizi bazalnim vrednostima nego u kontrolnoj grupi.
Koncentracija ova 4 jona, njihov sadrzaju u samome crevu kao i zapremina
crevnog sadrzaja su bili znacajno nizi u lecenoj grupi zivotinja.
Crevne histoloske promene su bile takodje blaze izrazene u tretiranih
zivotinja. Lecene zivotinje, hidrirane i nehidrirane su duze prezivljavale.
Kvantitativno izrazeno stepen i brzina varijacija promena ureje i
P u krvi su bili manji u oktreotidom tretiranih miseva.
ZAKLJUCI: SMS 201-995 ili oktreotid, kao jedino primenjeno farmakolosko
sredstvo tokom perioda revaskularizacije na eksperimenatalnom modelu sindroma
ishemije-revaskularizacije, je smanjivao zadrzavenje tecnosti u crevu,
odrzavao je procese crevne apropscije i sekrecije ( sa pozitivnim efektom
na intravaskularni prostor ) i smanjivao je tezinu crevnih ostecenja. Citoprotektivno
dejstvo, zastita od katabolickog stresa i sposobnost odrzavanja volemije
su bili u osnovi produzenja prezivljavanja zivotinja.
Kljucne reci: oktreotid, ishemija-revaskularizacija, crevo, prezivljavanje,
crevna apsorpcija-sekrecija.
INTRODUCTION.
The
polypeptide hormone somastotatin has different and multiple physiological
functions in the human body. Initially found to be a powerful inhibitor
of the growth hormone in the hypothalamus, somastotatin also fills
other important functions in different areas of the body.
Somastotatin inhibits gastrointestinal secretion by reducing the
secretion of Cl, Na and water into the intestinal lumen and increasing
the absorption of water and electrolytes from bowels (1,2). Other physiological
functions include the following: 1) intestinal blood flow by inhibiting
or stimulating intestinal neurons, 2) it produces an analgesic effect due
to its affinity with the opioid receptors, 3) it renews the intestinal
mucosa through its effects in the intestinal bowel crypts, 4) and it releases
or inhibits other gastrointestinal hormones such as vasoactive intestinal
peptide (VIP) (3,4,5). However, the clinical benefits of this hormone are
limited due to its short plasma half-life. Recently synthetic analogues
with the same biological effects and longer half-lives have been developed
one of these molecules is SMS 201-995.
The ischemia-revascularization intestinal syndrome is a time-depenent,
well-defined pathological entity within a patophysologic frame based in
two specific stages; the ischemic stage or hypoxemia and the revascularization
stage or the reintroduction of oxygen into the ischemic tissues. As a result,
the intestinal function of absortion-secretion, the blood flow, the cellular
integrity, the mucosa wall, its motility and the hormonal function of the
intestinal tract ara impaired.
Recently there has been a great number of research studies on the synthetic
analogue, the octreotide, and its role in the ischemia-revascularization
syndromes (6,7). On the another hand, other studies focused on the physiopathology
of this lesion and on the role of the SMS 201.995 in this pathology including:
cytoprotective effects, inhibitory effects on the pancreatic proteases,
and effects on the intestinal acid-based equilibrium (8,9,10).
Our hypothesis is that the SMS 201-995 or octreotide, a synthetic analogue
of the somatostatin has beneficial effects on acute ischemia-revascularization
syndrome and its pathophysiologic consequences. An experimental study has
been designed based on biochemical, clinical, histological and survival
data, in a protocol in which the octreotide is the only pharmacological
and therapeutical option.
MATERIAL AND METODS
Sixty
four male Wistar rats, weighging between 350-400 gr. were randomized in
four studies:
Biochemical clinic study. (From 20 animals, 10 had been treated
with octreotide and 10 with placebo). The study consisted of four stages:
Stage 1. The animals were housed for a week;
Stage 2. First
surgical operation was performed: an ischemic lesion was performed by temporary
ligation(90 min) with a clamp of the craneal mesenteric artery at
its bifurcation of the aorta . Before the ligation, basal blood rates of
Na, Cl, K and bicarbonate were measured; Stage 3. The observation
stage: 36 hours of observation during which the octreotide /Italfarmaco
SpA, Milan, Italy), was administered subcutatenously, 10 ug/100 gr. /8h
diluted up to 2 mL of saline, or placebo, 2 mL of saline only;
Stage
4. A second surgical operation: the quantitative data (venous concentration
of Na, Cl, K and bicarbonate) were recorded. After removal of the whole
length of the small bowel, the intestinal volume before and after centrifugation
of the guts and the intestinal concentration of Na, Cl, K and bicarbonate
were recorded. From this data the total intestinal content of the electrolytes
were obtained. Blood samples were taken from portal vein. All samples were
frozen after centrifugation to –80ºC and analized using
the same technique and reactives.
Histological and ultrastructural studies. ( 24 animals). The
intestinal content of 20 animals corresponding to the precedent study was
emptied. A segment of ileum was fixed in formol 6 % dehydrated and immersed
in paraffin, cuts of 5 um were obtained and stained with hematoxilin of
Harris-eosin, hematoxilin of Harris-floxin, PAS Schiff A-B and trichromic
with blue amiline according to the Masson tecnique and observed on an optic
microscope.
The remaining 4 rats followed the same protocol and split in two groups
of 2 (control and treated) but no quantitative nor qualitative data was
obtained. Once the intestinal segment was removed and fixed in glutaraldehide
2.5% and phosphate tamponade 0.1M,a specific treatment was performed before
being observed on the scanning microscope. This treatment involved cleaning
with tampon phosphate 0.1 M, dehydrating with acetone at increased concentrations,
drying with CO2 according to the critical point dryer method and coating
with coal of 400 A thick and gold. The readings of the samples on the optic
microscope were quantified with a score based on variables with increased
according the severity of the lesions:
•
Villi, according to the classification of Chiu and alies (11)
• The integrity of the musocal barrier.
• The type and quantity of inflammatory infiltrate and oedema
in
the lamina propia, submucosa, muscular, serosa layers.
• Dilatation of intrapariental vessels.
The readings of the samples on the scanning electronic microscope (Zeiss
DMS 940 A) were performed on an objective- comparative evaluation based
on four parameters: villi-number, size and shape-, apix of villi, stage
and type of mucosal secretion and bacterial flora and structure of the
brush border.
Survival studies with parenteral hydration. ( 20 rats, 10 with
octreotide, 10 with placebo). Three stages were carried out:
Stage 1.
The animals were housed for one week; stage 2. A surgical operation
similar to the lesion produced by the temporary ligation of the artery
on the previous study, catheterization of the external jugular vein and
measuring of the basal rates of inorganic phosphorus and plasmatic urea;
stage 3. The period to expiration of the animal (cardio-respiratory
arrest).During this last stage, the venous concentration of inorganic phosphorus
and the urea in blood samples of the tail veins were measured at
specific periods of time and the total period was noted.
The catheterization of the external jugular vein was performed with
an epidural catheter of 0.9 mm internal diameter and external of
1.5 mm and introduced down 3 to 3.5 cm according to with the animal weight.
The external connection to the infusion pump was with a Steffens model
(Alice King Chatham, Los Angeles CA and KDS 100, KDS Scientific Syringe
Pumps Inc Boston, MA). The infusion liquid introduced was a Ringer lactate
solution with 0.1 % bovine albumin at 0.25 ml/100 gr. weight/ hour for
both groups; the catheter was controlled daily. The drug and the placebo
were administered as in previous biochemical studies.
All samples were frozen after centrifugation to –80ºC
and analized using the same technique and reactives
4.Survival studies without parenteral hydration. ( 20 rats).
It included three stages: Stage 1: Animals were housed for
a week; Stage 2: A surgical interventions similar to previous studies
was performed; Stage 3: The survival period until the animals death.
No hydration nor control of inorganic phosphorus and urea were considered
in this study. Only the survival time until death ( cardio-respiratory
arrest) was accounted.
All
the rats were anaesthetised using Uretane 1.000 mg/kg weight intraperitoneally
every 6-8 hours. These studies followed the European regulations for research
purposes.
The
statistical analysis was different for each case. In the biochemical study,
the analysis of variance was used for quantitative data, and the
Fisher test for the statistical significance; the crossed diagrams
for the qualitative data and the student T test for the statistical differences
of histologic score. The Kaplan and Meier curves for the survival
studies and the Log Rank test for the Statistical significance. The urea
and the inorganic phosphorus rates were studied at two levels: 1. The variation
on serum quantitative data was observed by analyzing the urea under the
curve ( trapeze’s method) until the first death occurred; 2.
The variation on the velocity (line’s slope) of serum changes
by fitted equations to minimal models; in both cases the analysis of variance
and the Fisher test were used in order to find statistically significant
differences (p<0.01).
RESULTS
Biochemical
studies: No differences were obtained in the ionic serum values between
the treatment and the control group. The ionic serum rates obtained 36
hours after surgical lesion are indicated in TABLE 1: The Na in the treatment
and control groups was bellow the basal levels and no statistical
differences were observed between both groups of rats. The K rate
was over the basal levels for both groups, it being superior in the
control group than in the treatment group 36 hours after the surgical intervention;
a finding statistically significant. The Cloraemia was superior in the
control than in the treatment group; a result of important statistical
value. The bicarbonate mean value was below the basal level for both
groups; the control group showed a mean value lower than the treatment
group, with statistically significant differences.
TABLE
2 shows the statistics results of the chemical study of the guts. The intestinal
concentration of Na, K and Cl was lower in the treatment animals. The Na,
K, Cl total content was lower in the treatment group than the control.
The intestinal concentration and total content of bicarbonate was higher
in the treatment group than the control. The histological and ultrastructural
microfilms of 4 intestinal speciments are shown in FIGURES 1,2 . The histologic
score results were: 17 (2.46) for treatment group and 22.8 ( 2.46) for
control group. The Student’s T test was statistically significant
(p <0.0001). Then, animals treated with SMS 201-995 had less lesions
in their intestines respect to control animals.
The
survival studies results are shown in FIGURES 3,4,5,6. The mean survival
level was 197.0 hours for the hydrated treatment animals; 147.3 hours
for the non-hydrated treatment animals; 55.6 hours for the hydrated non-pharmacotreated
animals; and 41.9 hour for the non-hydrated, non-octreotide treated animals.
Significant differences were obtained in all groups. The Kaplan and Meier
survival curves for the four groups of animals with and without parenteral
hydration are shown in FIGURES 3,4.
The
statistics results of the studies with BUN and inorganic phosphorus are
presented in TABLE 3. The analysis of variance indicates that until the
first animal death in both groups, the total amount of BUN is higher in
the control than in the treatment group. Also, the amount of phosphorus
produced is higher in the control group. The BUN and the inorganic phosphorus
variation speed, represented by the curve gradients, were also faster in
the control group. FIGURE 5,6. All the differences were statistically significant.
DISCUSSION
This
study gives more information about the SMS 201-995 and its effects on the
guts in pathological situations.
According
to the biopharmacological base in which the octreotide uses the same mechanisms
as the biological somatostatin we have elaborated a pathological pattern
observed frequently in daily practice, the ischemia-revascularization syndrome;
the intestinal ischemias are generally non-obstructive; the
mesenteric hipoperfusion is the cause of intestinal ischemia in 10%
of cases; the hipovolemic shock and some surgical techniques like
transplants and aortic surgery also produce intestinal ischemia (12,13,14).
It has been observed that an ischemia of the guts lasting 90 to 120 minutes
produces sufficient damage to the viability of the affected gut (15).
Moreover any temporary intestinal ischemia induces changes in the gut like
disruption of the intestinal barrier and the subsequent alteration of the
bacterial flora producing systemic effects like sepsis (16).
In
our investigation the basal electrolytic values of the experimental animals
with the same breed and weight where within the normal limits, so no animal
was excluded from the research. Therefore all differences observed in the
treatment or control animals were due to the effect of SMS 201-995. Such
differences in treatment animals are outlined:
The intestinal absorption of Na, K and water are maintained.
The chloride secretion and intraluminal bicarbonate content are maintained.
The four electrolitic serum concentration investigated are closed to
the basal values.
The externa aspect of the intestinal villi is maintained. A minor lesion
of the villi, the inflammatory infiltrate and the oedema of the intestinal
layers.
The cytoprotective effect according to the rates of the intestinal phosphorus,
where the cellular ischemic lesion is of less degree and appears later.
According to the speed of production of BUN, the renal plasma flow subsequently
the plasma volume may have improved.
Alternatively the results obtained on the animal control are similar
to the ischemia- revascularization form. So the pharmacological effects
of the SMS 201-995 over this syndrome are evident. The octreotide effects
over the nonintestinal cases of ischemia-revascularization have been reported
by different authors (17,18).
The natural result of the ischemic grade is the end of the oxidative
phosphorilation, the decrease of the ATP and its function as the active
transport of the ATP. The ATP depletion produce Ca which is accumulated
on the internal surface of the plasmatic membrane, activating the ATPasa
Ca depenent and subsequently increasing the ATP depletion. The acumulated
Ca activates diverse phospholipases and proteases and produces disruption
on the plasmatic membrane and activates the intracellular proteolisis.
The ischemia produces a release of substances like histamine, VIP and
prostanoids and its effects increase the membrane permeability and the
apperance of the third space in the guts and subsequently the hipovolemia;
this increase of liquid produces intestinal distention and a decrease of
the mucosa vascularization due to compression. The ischemia also produces
lesions on the intestinal mucosa barrier as the pancreatic proteolisis
enzymes are released (19). All these elements produce alterations in the
intestinal barrier and changes in the bacterial flora and the absortion-secretion
intestinal processes will be effected (20).
The hypoxia and the absorption-secretion alterations of Cl/Na and H+/bicarbonate
will produce intestinal acidosis and therefore an increase of the bacterial
flora as well as alterations of the intestinal hemosthasia (21).The increase
of the bacterial flora maintains the intestinal lumen acidosis. The subsequent
toxemia will alter the intraparietal plexus causing an ileus paraliticus
and producing alterations in the absorption- secretions system (22,23).
As a result of the cellular hypoxemia, the proteolitic enzymes are released
and the bacterial toxemia will produce cellular lesions (23). As the intracellular
ions K and the inorganic phosphorus are released, their serum rate increase
(24). The hypovolemia, the decrease of the diuresis and the hypercatabolic
effect of the stress will icrease the BUN rates.
The results obtained from the investigations on the SMS 201- 995 and
their effects on the experimental animals are indicated in the changes
on the physiopathologic algorythm as shown in FIGURE 7:
The release of VIP is inhibited (25)
The proteases pancreatic release in inhibited (26)
The effects of the neurohumoral changes of the absorption-secretion
on the somatostatin receptors in the mienteric plexus, the submucosa and
the neurointestinal conexions are maintained (unconcluted research).
A cytoprotective effect due to: a) the cytoprotective prostanoid release
(27); b) the effects of the free oxygen radicals are diminished (28); c)
the cellular proliferation of the crypts and an increase exchange on the
intestinal cells due to the octreotide (the increase of LTB4); d)
a decrease on the plateled activity factor on the mucosa (9).
The blockage of Ca activity – by direct action or by modifying
the cAMP and cGMP cycles (4).
Regulation of the inflammatory response (23,29).
The influence on the intestinal motility (30,31).
All these actions permit:
To minimize the vasoactive effects of the medicators.
The maintenance of the peristalsis.
The alteration of the acid-base balance to be reduced to a minimum
as a overgrowth of the bacterial flora (as shown in the microfilms).
To minimize the hydroelectrolitic imbalance (as shown in the serum and
intestinal electrolytes rates).
During the evolution of the revascularization stage, the haemorrhange
on the
Intestinal lumen is observed , the hematocrit level decreases and emboli
are liberated with the risk of the animals death. It is believed nowadays
that the main cellular damage takes place during this stage and is due
mainly to the free oxygen radicals produced during the ischemic stage and
released during the revascularization stage (32,33).The cellular membrane
lesions will produce alterations in the intestinal absorption-secretory
system. Experimental studies demonstrate the effects of the octreotide
on the xantino-oxidase, that is, the effects of this molecule could alter
the response of the macrofagocyte on the lipopolysacarides, producing a
decrease of H2O2 and TNF secretion (29).A
cytoprotective effect has been attributed to this pharmacologic factor
due to the release of the free oxygen radicals (28). In our studies the
group of treatment animals persent better results than the control, that
id to say, the synthetic hormone has a clear effect on the cellular lesion
during the ischemia-revascularization: although this effect could be observed
in other studies during the ischemic stage (16), there is no evidence
of the pharmacological effect during the revascularization stage.
The
survival model proposed in this study consider the surgical lesion performed
as lethal, in other words, when the animal were left without completing
the treatment , the death was inevitable. This survival stage was considered
an important factor in the beneficial effects observed on the biochemic
and clinic studies demonstrating that the survival period was prolonged.
The study was divided in two parts: with and without parenteral hydration;
four different effects with two treatments were taken into account: without
hydration or octreotide, with hydration and octreotide, octreotide without
hydration, and hydration without octreotide. It was observed that the pharmacological
effects on the survival stage were positive both with or without hydration.
The
BUN, a factor which increased in the hypovolemic stage, proves a valuable
parameter on the renal hypoperfusion phase and therefore a good
indicator of the severity of the hipovolemic stage (34). Also as
a product of the proteic metabolism it indicates the degree of proteic
catabolism. Low rates of this metabolism on the treatment animals indicate
a better hydration and a better control of the proteic catabolism although
the survival rate is prolonged (35). The variation speed of the BUN in
the treatment animals is not lineal as it normally occurs in these pathology
but takes place in two stages:
Fast increase as in the control group.
Decrease.
It in effect shows that the pharmacological effects observed within
the first 36 hours during the biochemical-study ara maintained , improving
the renal function due probably to an increased volemia in response to
an increase of the absorption-secretion function of the guts.
The
inorganic phosphorus and the sulphates are the most important anions within
the intracellular compartment. In this work the inorganic phosphorus is
an indicator of the cellular necrosis, according to the high levels of
this ion on the intestinal ischemic processes (23,26).It gives information
about the cytoprotective effect of the octreotide as is shown
in our studies. Significant differences have been observed in the phosphoremia
between the treatment and the control group in the gap of timet
where all the animals were alive: in this period, the treatment animals
had lower levels of phosphoremia respect to control animals. This gap appears
at the beginning of the revascularization stage where the toxines increase
on the ischemic guts. The (line`s slope) of Pi presents the same curve
in the treatment and control group so the evolution of the phosphoremia
is similar in both groups but it appears later in the treatment group.
Therefore the pharmacological effects last until the death of the animals.
According to the previous studies the form of the curve (third degree
model) is as expected in this type of pathology (37).
The
octreotide treated animals, with or without hydration, present a better
survival rates and this could be due to:
A good hydroelectrolyte balance for a persistence of the intestinal
functions as the cellular integrity is maintained.
The control of the inflammatory reaction which otherwise leads
to a sepsis as it occurs in the necrohemorrhagic pancreatitis (38).
A decrease of the proteic catabolism and its side effects.
Therefore octreotide given during the revascularization stage as the
only treatment in the ischemic-revascularization syndrome and for a 90
min period total ischemia produces a decreases in the liquids retention,
maintains the Na, K intestinal absorption-secretion processes and has a
positive effect on the acid-basis intestinal balance. These pharmacological
properties improve the serum concentration of the four ions in the guts
which remain within the basal levels during the revascularization stage.
It also decreases the degree of intestinal lesions. In the long term
the octreotide has a cytoprotective effect, maintains an acceptable level
of volemia and decreases the proteic autodigestion during metabolic stress
on the revascularization stage. All these effects enables the prolongation
of cellular survival.
REFERENCES:
1. Rosenthal LE, Yamachiro DJ, Rivier J, Vale W, Brown M, Dharmsathaphorn
K. Structure-activity and relationships of somatostatin analogs in the
rabbit ileum and the rat colon. J Clin Invest, 1983; 71:840-9.
2. Anthone JA, Bastidas MS, Orandle MS, Yeo CJ. Direct proabsortive
effect of octreotide on ionic transport in thesmall intestine. Surgery,
1990; 108:2236-42.
3. Wood JD. Enteric neurophysiology. Am J Physol, 1984; 247: G585-98.
4. Carter RF, Bitar KN, Zfass AM, Makhlouf GM. Inhibition of
VIP-simulated intestinal secretion and cyclic AMP production by somatostatin
in the rat. Gastroenterology, 1976; 74; 726-30.
5. Harris AG. Future medical prospectives for Sandostatin. Metabolism,
1990; (suppl 2): 180-5.
6. Usadel KH, Schewedes U, Wdowinski JM. Pharmacological effects of
somatostatin in acute organ lesions. Inn Med, 1992; 9: 204-9.
7. MT Fallon. The physiology of somatostatin and its synthetic analogue,
octreotide. Eur J Pal Care, 1995; 1:18-22.
8. Mulhivil S, Pappas TN, Passaro E, Debas HT. The use of somatostatin
and its analogs in the treatment of surgical disorders. Surgery,
1986; 100: 467-75.
9. Eliakim R, Karmeli F, Rachmilweitz O. Octreotide effectively decreases
mucosal damage in experimental colitis.. Gut, 1993; 34:264-69.
10. Soudah HC, Hasler WI, Owyang C. Effects of octreotide on intestinal
motility and bacterial overgrowth is sclerodermia. New Eng J Med, 1981;
325:1461-7
11. Chiu CJ. Intestinal mucosa lesions in low flow states. I.
A morphological, hemodynamic and metabolic reapprisal. Arch Surg, 1970;
101: 478-85.
12. Pless J, Bauer W, Briner U. Chemistry and pharmacology of SMS 201-995,
a long acting octapeptide analogue of somatostatin. Scand J Gastroenerol,
1986, suppl; 21:54-64.
13. Clavien P, Harvey PRC, Strasberg SM. Preservation and reperfusion
injuries in liver allografts: An overview and synthesis of current studies.
Transplantation, 1992; 53:957,63.
14. Glower DG, Wolfe WG. Management of dissecting aortic aneurysms.
In Yao JST, Perace WH (eds.): Aneurysms: New findings and treatment. East
Norwalk, Con., Appleton & Large, 1994.
15. Ottinger LW. Mesenteric ischaemia. N Engl J Med, 1982; 307:535-39.
16. JL Landa, M Gomez, A Moreno, L Llanos, M Quadros, JL Balibrea. Citoprotective
effects of somatostatin (SS) in a rat model of hepatic ischemia- reperfusion.
J Hepatology, 1991; 13 (suppl 2):42.
17. Parks DA, Granger DN. Ischemia- reperfusion injury: radical review.
Hepatology , 1988; 8:680-2.
18. Hoffmann TF, Uhl E, Messmer K. Protective effect of the somatostatin
analogue octreotide in ischemia/ reperfusion- induced acute pancreatitis
in rats. Pancreas, 1996; 12: 286-93.
19. Bounous G. Release of intestinal enzymes in acute menesteric ischemia.
J Surg Res, 1969; 9:339-47.
20. Saandia R, Schein M, MacFarlane C, Boffard KD. Gut barrier function
and the surgeon. Br J Surg, 1990; 77:487-92
21. Anderson R, Parson H, Isakson B. Acute intestinal ischemia. Acta
Chir Scand, 1984; 150:217-36.
22. Marston A, Clarke JMF, Garcia JG. Intestinal function and
intestinal blood supply: a 20 year surgical study. Gt, 1985;260:656-9
23. Karalis K, Mastokaros G, Chrousos, Tolis G. Somatostatin analogues
suppress the inflammatory reaction in vivo. J Chin Invest, 1994; 93:2000-2006.
24.Ferentis CB, Koborozos BA, Vyssouslis GP,Manouras AJ,Apostolodis
NS, Golematis BCh. Serum phosphatase levels in acute bowel ischemia. An
aid arly diagnosis. Am Surg, 1985; 51: 242-6.
25. Nelgard P, Bojo L, Cassuto J, Importance of vasoactive intestinal
paptide and somatostatin for fluid losses in small-bowel obstruction. Stand
J Gastroenterol, 1995; 30: 464-69.
26. Lamberts SW, van der Lely AJ, de Herder WW, Hofland LJ. Octreotide.
N Engl J Med, 1996; 334: 246-54.
27. Sikujara O, Mondem M, Toyoshima K, Okamura J, Kosali G. Citoprotective
effects of prostaglandin 12 on ischaemia- induced hepatitis cell injury.
Transplantation, 1983; 36:238-42.
28. Morris JB, Guerrero NH, Furth EE, Stellato TA. Somatostatin attenuates
ischemic intestinal injury, Am J Surg, 1993; 165:676-80.
29. Chao TC, Cheng HP, Walter RJ. Somatostatin and macrophage function:
modulation on hydrogen peroxide,nitric oxide and tumor necrosis factor
release. Regul Pept, 1995; 58: 1-10
30. Cullen JJ, Eagon JC, Kelly KA. Gastrointestinal peptide hormones
during postoperative ileus. Effect of octreotide. Dig Dis Sci, 1994; 39:
1179- 84.
31. Poitras P, Trudel L, Miller P, Gu CM. Regulation of motilin release:
studies with ex vivo perfused canine jejunum. Am J Physiol, 1997; 272:
G4-9.
32. Parks DA, Granger DN. Ischaemia-induced vascular changes: Role of
xanthine oxidase and hydroxil radicals. Am J Physiol, 1983; 245: G285-9.
33. Parks DA, Shah AK, Granger DN. Oxygen radicals: effects on intestinal
vascular permeability. Am J Physiol, 1984;247:G167-70.
34. Tilney NL, Morgan AP, Lazarus JM. Acute renal failture in
surgical patients. In: Tilney NL,Lazarus JM (eds): Surgical care of the
patient with renal failure. Philadelphia, WB Saunders Co, 1982.
35. Shaw JHF, Wolfe RR. Metabolic intervention in surgical patients.
Ann Surg, 1987; 207: 274-82
36. Jamieson WG, Lozon A, Durand D, Wall W. Changes in serum phosphatase
levels associated with intestinal infarction and necrosis. Surg Gynecol
Obstet, 1975;140:19-21
37. Karmierczak SC, Lott JA, Caldwell JH. Acute intestinal infarction
or obstruction: search for better laboratory tests in an animal model.
Clin Chem, 1988;34: 281-8.
38. Fieldser F, Jaurnig G, Keim V,Richter A, Bender HJ. Octreotide
treatment in patients with necrotizing pancreatitis and pulmonary failure.
Intensive Care Med, 1996; 22: 909-15.
TABLE 1
Biochemic-clinic study. The serum ions result in mEq/L –media
(SD)- in the treatment and control groups during the first and second operation
and their ststistic differences.
|
FIRST INTERVENTION
|
Na
|
K
|
Cl
|
Bicarbonate
|
|
TREATED
|
139. 30 (0.76)
|
5.98 (0.13)
|
100.16 (1.16)
|
25.99 (0.40)
|
|
CONTROL
|
140.16 ( 2.86)
|
5.04 (0.13)
|
100.30 (1.34)
|
26.82 (0.65)
|
|
Fisher’s test value
|
0.26
|
1.11
|
0.74
|
0.70
|
|
Pvalue
|
<0.99
|
<0.36
|
<0.69
|
<0.73
|
|
SECOND INTERVENTION
|
|
Na
|
K
|
CL
|
Bicarbote
|
|
TREATED
|
139.89 (3.49)
|
5.67 (0.28)
|
114.98 (3.54)
|
22.33 (2.58)
|
|
CONTROL
|
143.80 (2.78)
|
9.13 (0.22)
|
133.13 (3.39)
|
17.36 (1.33)
|
|
Fisher’s test value
|
5.13
|
132.26
|
26.98
|
22.84
|
|
Pvalue
|
< 0.02
|
< 0.0001
|
< 0.0001
|
< 0.0001
|
TABLE 2
Biochemic- clinic studies. Intestinal ions result – media
(SD)- cencentration (mEq/L) and total content (mEq) and the intestinal
volume (before and after centrifugation) in mL and their statistics differences
in the treatment and control animals.
|
Concentration (mEq/L)
|
TREATED
|
CONTROL
|
Fisher’s Test Value
|
P value
|
Na
|
124.36 (2.98)
|
142.36 (1.82)
|
27. 70
|
<0.0001
|
|
K
|
7.36 (0.58)
|
17.49 (1.28)
|
294.14
|
<0.0001
|
|
Cl
|
105.31 (4.06)
|
114.28 (2.76)
|
8.37
|
<0.0046
|
|
Bicarbonate
|
24.34 (2.15)
|
10.01 (1.32)
|
322.04
|
<0.0001
|
|
Intestinal content (mEq)
|
TREATED
|
CONTROL
|
Fisher’s Test Value
|
P value
|
Na
|
0.40 (0.03)
|
1.03 (0.06)
|
57.09
|
<0.0001
|
|
K
|
0.023 (0.003)
|
0.125 (0.006)
|
178.26
|
<0.0001
|
|
Cl
|
0.341 (0.03)
|
0.830 (0.04)
|
38.24
|
<0.0001
|
|
Bicarbonate
|
0.127 (0.03)
|
0.067 (0.01)
|
54.42
|
<0.0001
|
|
Intestinal volumen (mL)
|
TREATED
|
CONTROL
|
Fisher’s Test Value
|
P value
|
Before centrif
|
13. 25 (1.85)
|
17.35 (2.48)
|
16.09
|
<0.0001
|
|
After centrif
|
5.25 ( 1.25)
|
6.67 (1.04)
|
7.30
|
<0.008
|
TABLE 3
Survival study. The analysis of variance results with the inorganic
phosphorus and BUN data: A. Quantitative grade of the variation (mean (SD))
and B. Velocity of variation - curve’s slope- (confidence
intervals of the curves’ angular coefficient). (The quantitative
grade of the variation obtained according the area below de curve- until
the first animal dead- according to the trapeze’s rule; the velocity
of variation has been studied with equations fitted to minimum models
and each section of the resultant curve has been compared- using the confidence
intervals of the angular coefficients of the curves- between treatment
and control animal, to check if the sections were overlaped).
Legent: Beta 0 (curve value in the Y axis); Beta 1 ( time and section
1 of the curve); Beta 2 (time and section 2 of the curve); Beta 2 (time
and section 2 of the curve); Beta 3 (time and section 3 of the curve).
A.
|
AREA BUN
|
AREA Pi
|
TREATMENT
|
174.10 (3.37) |
93.34 (5.34) |
| CONTROL |
794.25 (30.80) |
428.82 (45.50) |
| Fisher’s test value |
488.11 |
536.22 |
| P value |
<0.0001 |
<0.0001 |
B.
|
TREATMENT |
CONTROL |
P of no-overlaped |
BUN
|
|
|
Beta 1
|
0.003602+/-0.000011
|
0.036344+/-0.004605
|
P<0.01
|
|
Beta 2
|
-0.0000169+/-0.00004
|
----
|
----
|
|
Pi
|
|
|
Beta 1
|
0.039939+/-0.003992
|
0.153388+/-0.019671
|
P<0.01
|
|
Beta 2
|
-0.000460+/-0.000046
|
-0.003841+/-0.000844
|
P<0.01
|
|
Beta 3
|
0.00000013+/-0.00000015
|
0.000325+/-0.0000096
|
P<0.01
|
FIGURES
 A
A 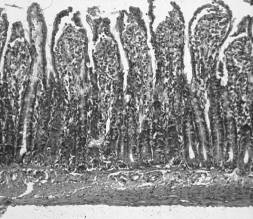 B
B
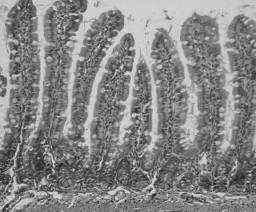
FIG 1. Microfilms of a segment of ileum of the animals treated
with octreotide (A) and the control (B). The ischemic lesion
grade 1 (according to Chiu classification (11)) in the intestinal
villi are evident in (A); the mucosal barrier is fairly intact;
an acute inflamatoy infiltrate, oedema of the lamina propia and submucosa
appears; mild vasodilation at all celular levels; no haemorrhage is observed.
Ischemic lesions grade 3 are observed on the villi (B); the mucosal
barrier is impaired and the axial sides of the villi are conserved; an
important inflamatory infiltrate and oedema appear on the lamina propia
and submucosa; moderate vasodilation at all levels (Hemtaxylin of Harris-eosine,
x 20).
 A
A 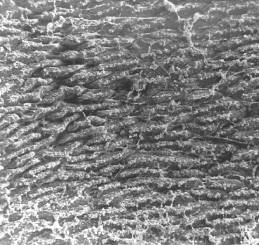 B
B 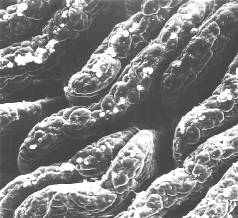 C
C 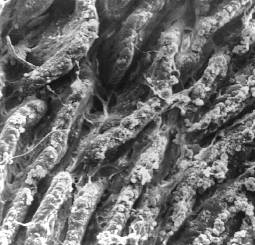 D
D
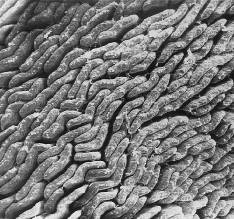
FIG 2. Microfilms taken from a scanning electronic
microscope of the ileum segment of one of the animals treated with octreotide
(A,B), and the control grup (C, D). An opening of the villi
apex, remarkable bacterial overgrowth, changes on the bacterial flora and
red blood cell diapadesis are observed in C and D; therefore
a celular substance from lamina propia is secreted through the open villi;
the mucus secretion is absent. The external aspect of the villi shows a
normal aspect and the mucus secetion is abundant, the bacterial overgrowth
is moderate (A,B). (A and C, x 50; B and D, x 200).
FIG 3. Kaplan and Meier curves on the treatment and
control animals in the survival studies with parenteral hydration.
FIG 4. Kaplan and Meier curves on the treatment and control animals
in the survival studies without parenteral hydration.
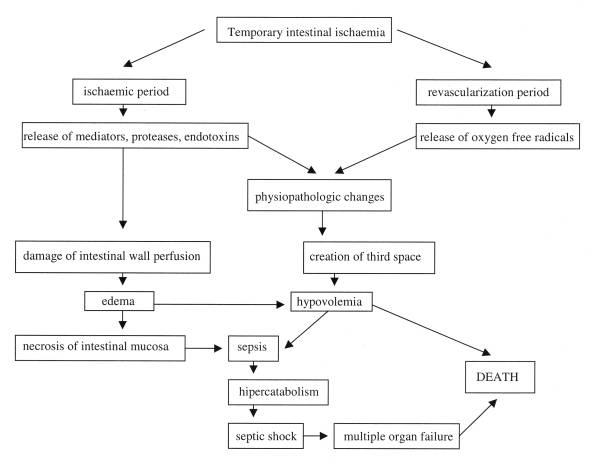
FIG 5. Curves according data fitted at minimun models; Velocity
of variation (line's slope) of BUN in the treatment and control animals.
FIG. 6. Curves according data fitted at minimun models; Velocity of
variation (line's slope) of Pi in the treatment and control animals.
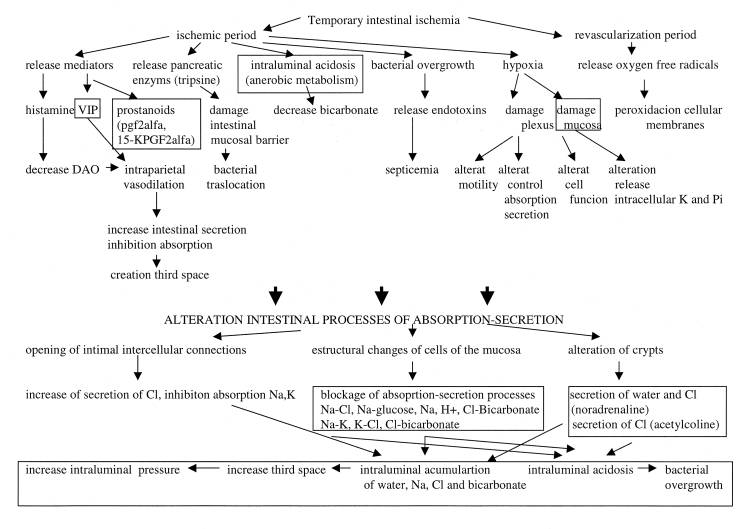
FIG 7. Algorythm of physiopathologic events in the intestinal ischemia-revascularization.
The frames shows the levels where the octreotide could have an effect.
Legend: Bic: bicarbonate; DAO: diaminoxydase; VIP: vasoactive intestinal
peptide; PGF: prostaglandin F.