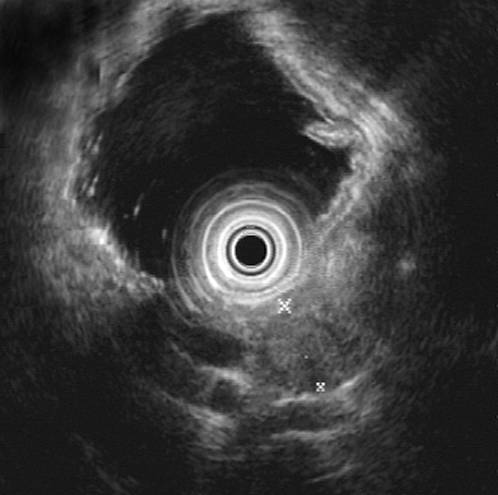
Figure 1. EUS of insulinoma in pancreatic body: hypoechoic tumor with
echo-free halo.

Alimentarni trakt i pankreas
ARCH GASTROENTEROHEPATOL 2001; 20 ( No 3 - 4 ):
Case report
Insulinoma by endoscopic ultrasound: A case report
Endoskopski ultrazvuk insulinoma: Prikaz slučaja
( accepted December 23rd, 2001 )
1MiodragN.Krstić, 2Aleksandra Kendereški, 2Aleksandar Diklić, 2Dragan Micić, 1Predrag
Dugalić, 1Dragan Tomić, 1Aleksandra Pavlović.
1Institute of Digestive Diseases, Clinical Center of Serbia,
Belgrade,
2Institute of Endocrinology, Clinical Center of Serbia, Belgrade.
Abbreviations use in this article: EUS, endoscopic ultrasound; US, ultrasound;
CT, computed tomography, MRI, magnetic resonance, FNA, fine needle aspiration.
Address correspondence to: Docent Dr Miodrag N. Krstic, Sci D.
Clinic for Gastroenterology and Hepatology,
Institute of Digestive Diseases,
Clinical Center of Serbia,
Koste Todorovica 6 St.
YU-11000 Belgrade, Serbia, Yugoslavia
E-mail:miodrag [email protected]
ABSTRACT
Preoperative localization of pancreatic neuroendocrine tumours is difficult. Noninvasive, imaging methods such us abdominal US, CT or MRI are not sensitive enough as well as selective angiography According to the literature data it appears that EUS is fare more accurate than any other diagnostic method in the preoperative localization of pancreatic neuroendocrine tumours. Here we report the very first case of insulinoma preoperatively localized by EUS in our country. The role of various diagnostic modalities in detecting small pancreatic neoplasms is discussed in a detail.
Key words: Insulinoma, endoscopic ultrasound.
SAŽETAK.
Preoperativna lokalizacija neuroendokrinih tumora pankreasa je obično teška. Neinvazivni dijagnozni testovi kao što su abdominalni UZ, CT ili MRI ne pokazuju dovoljnu osetljivost u dokazivanju malih tumora. Isto se odnosi i na selektivnu angiografiju. Po literaturnim podacima, EUS je daleko precizniji od svih drugih dijagnoznih modaliteta u preoperativnoj lokalizaciji neuroendokrinih tumora pankreasa. U radu je prikazan prvi slučaj inzulinoma koji je u našoj zemlji preoperativno dokazan endoskopskim ultrazvukom. U radu je takodje do detalja diskutovana uloga pojedinih dijagnoznih modaliteta u detekciji malih pankreasnnih tumora.
Kljucne reci:: Insulinom, endoskopski ultrazvuk.
INTRODUCTION
Insulinomas are the most common pancreatic neuroendocrine tumours.(1) Its preoperative localization is very difficult (2). Noninvasive, imaging methods, such us abdominal UC, CT or MRI are not sensitive enough (3). On the contrary supraselective angiography has higher diagnostic yeald, but significant proportion of tumours still remain of undetermined origin (1). Here we report the very first case of insulinoma preoperatively localized by EUS in this country. The role of various diagnostic modalities in detecting small pancreatic neoplasms is discussed.
REPORT OF A CASE
A 34-year old woman was admitted to the Institute of Endocrinology, Clinical Center of Serbia, because of numerous repeated episodes of sweating, shaking, nervousness, and agitation. First episode was recorded eight months before admission. At that time her blood sugar was 2.8 mmol/l. Ten days before admission she lost consciousness while blood sugar was 2.3 mmol/l. The weight gain during whole period was 10 kg.
At admission her physical examination was unremarkable, BMI 30.5 kg/m2, BP 120/80mmHg, puls rate 80/min. Glycemia was 2.0 mmol/l. Routine laboratory examinations were normal including serum calcium and phosphate concentration, except iron deficiency anemia which was successfully treated. 5-hour oral glucose tolerance test (OGTT) demonstrated basal hypoglycemia which persisted during the test. Basal insulinemia was inadequately elevated in comparison to the basal glycemia. Table 1. During fasting test hypoglycemia was found on the beginning and persisted throughout the whole test, which was terminated after 7 hours. During the test I/G index (insulinemia/glycemia ratio) was elevated indicating organic hyperinsulinism. Table 1. At the end of fasting test acetonuria was negative, and plasma cortisol level was 537 nmol/l. I/G index was also elevated (0.54) during spontaneous hypoglycemic attack. Insulin suppression test was terminated after 60 minutes because of serious hypoglycemic symptoms (agitation). Glycemia was 1.9 mmol/l on the beginning and 0.4 mmol/l at the end of the test, with suppression of plasma C-peptide level of 37.5 % at the end of the test, confirming the diagnosis of organic hyperinsulinism.
Abdominal US and MRI examination were normal.
EUS of the pancreas showed in the distal part of pancreatic body hypoechogenic, well demarceted structure, 15.8 mm in diameter. Figure 1.This lesion was of similar echo structure as normal pancreatic tissue. Black halo separated it from the rest of pancreas.
Radiographic examination of chest and sella turcica showed normal findings. ECG showed no abnormalities. Basal hormonal status was normal.
Patient was diagnosed as having insulinoma and operated upon. Intraoperatively tumour 2 cm in diameter was found in the body of the pancreas, and distal pancreatectomy with splenectomy was performed. Figure 2. Histology of resected tumour was diagnostic for insulinoma. Postoperative recovery was unremarkable. Postoperatively blood sugar concentrations during the 24-hour glucose profile determination were normal and OGTT as well Table 2. The patient has remained euglycemic 10 months after tumour resection.
DISCUSSION
The diagnosis of neuroendocrine neoplasms is based on symptomatology, signs, functional tests, and hormone essays (4). Among various neuroendocrine pancreatic tumours, gastrinomas and insulinomas are fare more common than glucagonoma, somatostatinomas, or VIPomas. (1). Insulinomas are generally small (>90% are <2 cm in diameter), usually solitary (90%); 5-15% are malignant (5) They are almost invariably pancreatic, distributed equally in the pancreatic head, body and tail (5). On the contrary to insulinoma, gastrinomas are in 30-45% of cases extrapancreatic (duodenal wall, lymph node, liver) (1) At the time of diagnosis the average age of insulinoma patients is between 40-50 years. More than three quarter of insulinomas can be localized at surgery by palpation and intraoperative ultrasonography (5). The precise preoperative localisation of the pancreatic neuroendocrine tumour is necessary to confirm the diagnosis and facilitate surgery (1-5).
In patients suspected as having pancreatic neuroendocrine tumours, noninvasive imaging tests should be performed at first: abdominal CT, US, and MRI. These procedures at best locates only 40-60% of functional neuroendocrine tumours (3). In the majority of cases small insulinomas and gastrinomas cannot be identified (2). This was confirmed in our case in which abdominal US and MRI were negative. Octreotide scanning with iodine-123 or indium 111- labeled octreotide is highly sensitive in diagnosing gastrinomas ( 80-90%) (1,4). However, insulinomas have fewer somatostatin receptors what lowers sensitivity of insulinoma detection (4). Selective angiography may identify neoplasams not evident on dynamic CT. Transhepatic portal venous sampling may help in localizing affected region of the pancreas (5) However, this method is tehnically demanding, invasive, expensive and frustrating number of tumors remain occult.
EUS was intially designed in order to improve the detection of the
small pancreatic carcinoma (6,7). It has been well demonstrated that EUS
allow careful imaging of the pancreas through the wall of the duodenum
and stomach (8-12) Thus, it was logical to apply this method for localization
of pancreatic neuroendocrine tumors which are small. Small endocrine pancreatic
tumorus, even as little as 4mm, could be visualised by EUS (13-14). Endocrine
tumours usually appears as homogenous, hypoechogenic masses with smooth
margins (1). Some authors described an echo-free halo around the tumor
(17). Our patient had such tumour with clearly visualized dark halo. On
the other hand, some tumours are echo-rich or with pattern almost the same
as surrounding tissue.
Ten years ago, large multicentric study was performed to determine the ability of EUS do detect pancreatic neuroendocrine tumours in patients with negative CT and US (18). Overall sensitivity of EUS was 82% and specificity 95%. EUS was significantly more sensitive than angiography (82% vs 27%) (18). This was later confirmed by several groups confirming that EUS is a highly accurate modality for the localization of the pancreatic endocrine tumors, with the sensitivity between 82 and 89% (19-22). It has been shown in case-control study that EUS significantly reduces charges for preoperative localization studies ($ 2620 vs. 4846$), largely due to a decrease in the number of diagnostic angiograms and venous sampling procedures, and also reduced surgical and anesthesia times (23). Preliminary reports found that EUS guided fine needle aspiration may significantly increase the accuracy rate of EUS for the detection of endocrine tumors (24-26).
In conclusion, we demonstrate for the first time in this country that insulinoma
may be diagnosed preoperatively by EUS, despite the negative MR and conventional
abdominal US. In experienced hands, this is highly accurate diagnostic
method for the localiazation of pancreatic endocrine tumors. EUS has to
be performed when standard noin-invasive imaging procedures are not conclusive
or negative.
Table 1.
PREOPERATIVE RESULTS
|
|
|||||||||||||||||
| Time (min) | 0 | 30 | 60 | 90 | 120 | 150 | 180 | 240 | 300 | ||||||||
| Glycemia (mmol/l) | 2.0 | 1.8 | 1.5 | 3.0 | 1.5 | 1.8 | 2.3 | 2.4 | 2.2 | ||||||||
| Insulinemia (mU/l) | 13.8 | 116.6 | 26.8 | 95.7 | 17.9 | 12.7 | 13.9 | 6.2 | 6.7 | ||||||||
| C-peptidemia (nmol/l) | 0.19 | 0.32 | 1.12 | 8.3 | 6.1 | 11.1 | 10.2 | 6.0 | 8.4 | ||||||||
FASTING TEST |
|||||||||||||||||
| Time (hours) | 06 | 07 | 08 | 09 | 10 | 11 | 12 | 13 | |||||||||
| Glycemia | 1.1 | 1.3 | 1.5 | 1.8 | 2.3 | 1.7 | 1.5 | 1.8 | |||||||||
| Insulinemia | 31.5 | 21.6 | 10.l | 10.l | 11.9 | 20.2 | 10.9 | 8.9 | |||||||||
| I/G index | 1.59 | 0.92 | 0.37 | 0.31 | 0.28 | 0.66 | 0.4 | 0.17 | |||||||||
| C-peptidemia | 0.47 | 0.39 | 0.21 | 0.10 | 0.23 | 0.4 | 0.19 | 0.10 | |||||||||
INSULIN SUPERESSION TEST |
|||||||||||||||||
| Time (min) | 0 | 30 | 60 | ||||||||||||||
| Glycemia | 1.9 | 1.3 | 0.4 | ||||||||||||||
| Insulinemia | 1.8 | 57.5 | 50.0 | ||||||||||||||
| C-peptidemia | 0.168 | 0.118 | 0.105 | ||||||||||||||
Table 2.
POSTOPERATIVE RESULTS
|
|
|||||||||
| Time (hours) | 08 | 10 | 12.30 | 15 | 18 | 20 | 24 | 03 | 08 |
| Glycemia | 5.2 | 5.4 | 4.9 | 6.2 | 5.8 | 4.2 | 5.5 | 4.8 | 4.4 |
|
|
|||||||||
| Time (min) | 0 | 30 | 60 | 90 | 120 | ||||
| Glycemia | 3.7 | 5.9 | 5.1 | 3.4 | 4.1 | ||||
| Insulinemia | 12.3 | 19.7 | 63.1 | 25.3 | 29.2 | ||||
Figure 1. EUS of insulinoma in pancreatic body: hypoechoic tumor with
echo-free halo.
REFERENCES: