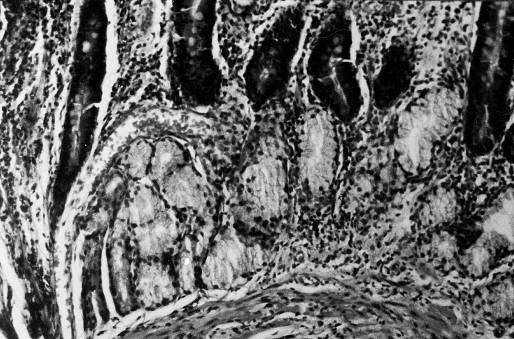
Figure 1. Chronic duodenitis with extensive gastric metaplasia ( HE x 250).
ARCH GASTROENTEROHEPATOL 2001; 20 (No 3 – 4):
1Saša Grgov*, 2Milosav Stefanovic,
3Vuka
Katic i 4Tomislav Tasic.
1Department of Medicine - Unit of Gastroenterology, Health
Center Leskovac, 2Department of Pathology, Health Center Leskovac,
3Institute
of Pathology, Clinical Center Niš, 4Clinic of Gastroenterology
and Hepatology, Clinical Center Niš, Serbia, Yugoslavia.
Abbreviations used in this article:
DU, duodenal ulcer; GM, gastric metaplasia; H. pylori,
HP.
Address correspondence to: Primarius Dr Saša Grgov, Sci
D.
Department of Medicine - Unit of Gastroenterology,
Health Center Leskovac,
Svetozara Markovica 116 Str.
YU-16000 Leskovac, Serbia, Yugoslavia
Fax. + 381 16 247810.
H.pylori, gastric metaplasia, duodenum Gastroenteroloska sekcija SLD-
01714,2001.
*Dr Sasa Grgov is new appointed member of the Editorial Board of the Archives of gastroenterohepatology.
Upper gastrointestinal endoscopy was performed in 125 consecutive patients: 70 with duodenal ulcer and 55 controls. Rapid urease test and antral gastric biopsies were used for detection and semiquantitative assessment of H. pylori presence. In order to diagnose duodenal gastric metaplasia in biopsy specimens, hematoxylin-eosin and periodic acid Schiff staining method were used. We were unable to rely the prevalence and the extent of duodenal bulb gastric metaplasia with H. pylori antral colonisation rate and degrees of its antral colonisation density. We found that duodenal gastric metaplasia was more frequent in duodenal ulcer patients than in controls (55.9% vs. 25%, p < 0.05, for H. pylori positive and 72.7% vs. 33.3%, p < 0.05, for H. pylori negative patients). We conclude that H. pylori is not an obligatory factor in the aetiology of duodenal gastric metaplasia, nor the factor of the extension of already present gastric metaplasia. Duodenal ulcer itself is a key denominator of duodenal gastric metaplasia.
Key words: H. pylori, duodenal ulcer, gastric metaplasia.
Gornja gastrointestinalna endoskopija je nacinjena kod125 pacijenata, 70 sa duodenalnim ulkusom i 55 pacijenata kontrolne grupe. Za otkrivanje i semikvantitativnu procenu H. pylori koriš?en je ureaza test i histološki pregled antralne sluznice. Radi histološkog ispitivanja gastri?ne metaplazije u duodenumu primenjeno je hematoxylin-eozin i periodic acid Schiff bojenje. Rezultati istraživanja su pokazali da se prevalencija i ekstenzitet gastri?ne metaplazije u bulbusu duodenuma nije bitno razlikovala u odnosu na H. pylori status u želucu, kao ni po stepenima denziteta H. pylori kolonizacije u antruma. Utvr?ena je statisti?ki zna?ajno ve?a u?estalost gastri?ne metaplazije kod pacijenata sa duodenalnim ulkusom, u odnosu na kontrolnu grupu (55.9% prema 25%, p < 0.05, za H. pylori pozitivne i 72.7% prema 33.3%, p < 0.05, za H. pylori negativne pacijente). Zaklju?ujemo da H. pylori nije obavezan ?inilac nastanka gastri?ne metaplazije, niti faktor ekstenzije ve? prisutne gastri?ne metaplazije. Duodenalni ulkus je dobar pokazatelj prisustva gastri?ne metaplazije.
Klju?ne re?i: H.pylori, duodenalni ulkus, gastri?na metaplazija.
INTRODUCTION
The origin of duodenal gastric metaplasia (GM) in the proximal part of the duodenum is far from fully elucidated. Using three-dimensional reconstructions of villi based on serial sections of duodenal mucosa it is demonstrated that, after originating in Brunner’s glands ducts, metaplastic cells migrate as a tight cohort, or column, up the villus. Therefore GM cells are identical to the cells from Brunner’s gland ducts according to the content of mucus, bicarbonate, epidermal growth factor, and trefoil peptide (1,2,3). According to Kushima et al. a new generative zone, "neo G zone", is formed in Brunner’s glands in the presence of duodenitis and duodenal ulcer (DU) (4,5). This zone produces M1-positive foveolar cells, which migrate towards the lumen with elongation of the generative zone and gastric gland formation. Histologically, GM cells contain neutral mucins and can be detected by PAS staining. Electromicroscopically, metaplastic cells contain numerous apical mucous drops characteristic for superficial gastric mucous cells (6).
Since H. pylori (HP) colonises only the gastric type
of epithelium, the presence of GM in the duodenum makes the bacterial colonisation
of the duodenum possible. Data about potential role of HP in the
production of GM in the duodenum are controversial (6, 7,8, 9).
The aim of this prospective study is to assess the role of
HP
infection in the occurrence of GM in the duodenum, as well as to examine
the relationship between GM and DU.
The criteria for exclusion of the patients from the study were as follow: 1) therapy with proton pump inhibitors and antibiotics during the past four weeks, and prolonged nonsteroidal anti-inflammatory drugs medication; 2) previous stomach surgery, with the exception of simple sutures because of ulcer perforation; 3) excessive long-lasting alcohol ingestion; 4) pregnancy and lactation; 5) active ulcer bleeding; 6) peptic stenosis of the duodenum; 7) severe associated diseases; 8) data about previous ulcer disease in the control group of patients with non-ulcer dyspepsia.
Endoscopy and biopsy After six-hour fasting, disinfection of the instrument, and local pharyngeal anesthesia with 10% xylocain upper GI endoscopic examination with mucosal biopsies were performed. Two gastric mucosal biopsies were taken for rapid HP urease test (antral plus fundic) and 6 biopsies for histologic examination (3 from the antrum, at least 20 mm from the pylorus, from the anterior and posterior walls and from the incisura angularis, and 3 biopsies from gastric corpus/fundus- the anterior and posterior wall).
In order to examine the presence HP and GM in the duodenum,
mucosal biopsies were taken from the anterior wall of duodenal bulb for
rapid urease test and 4 biopsies for the histologic examination (anterior
and posterior wall, as well as from the margins DU if present)
To avoid or reduce the possibility of cross-contamination, the biopsy
forceps were washed up with water whenever biopsy forceps passed from one
segment of mucous membrane to another.
HP status was considered positive when both tests were positive
(rapid urease test and histologic examination).
The result of the urease test was read after 1, 3 and 24 hours. The
test was regarded positive if colour was changed from yellow to red.
For identification and semiquantitative evaluation of HP status by histology, endoscopic mucosal biopsy samples were fixed in 10% formalin for 24 hours. After that tissue specimens were embedded in paraffin, and cut by microtom up to the thickness of 4 µm. After the deparafinisation and processing in graded alcohol, selected clippings were stained by hematoxylin-eosin (HE) and Giemsa. HP antral colonisation density was determined semiquantitatively in the interval from 0-3 (0, absence of HP; 1, small number of HP focally; 2, large number of HP focally or small number, diffusely; 3, a large number of HP diffusely) (8). During histologic evaluation, the pathologist was not informed about urease test.
To explore GM in the duodenal bulb, HE and PAS (Periodic Acid Schiff) staining were used. Figure 1. When duodenal GM was present, focuses of gastric antral type mucosa were verified in the bulb. Their epithelial cells contained PAS positive fucomucines in the apical part of the cytoplasm. Figure 2. The extent of GM in duodenal mucosal biopsy specimens was scored from 1 - 4: 1, GM found in less than 5% of the surface of the duodenal mucosal surface; 2, 5-20% GM; 3, 21-50% GM; 4, > 50% GM (10).
Statistic analysis The results are presented tabularly and graphically according to the methodology of descriptive statistic. In order to verify the hypotheses and determine the significance of the differences between certain parameters, specific statistic tests were used, such as Mantel-Haenszel’s c2 test with Yates’s correction, Fisher’s test of exact probability of zero hypothesis and Student’s t test. In addition, for analysing the independent data groups, when the variation coefficient was larger than 30%, Mann-Whitney U-Wilcoxon Rank Sum W test was used.
The differences between certain parameters were considered significant
for values p < 0.01 and p < 0.05, and not significant for values
p > 0.05. We also calculated the relative ratios and risk indices, such
as cross-ratio or odds ratio (OR) and relative risk (RR), with the confidence
interval of 95% (95% CI).
In HP negative patients GM was statistically much more frequent
in DU patients (72.7%) than in the controls (33.3%) p < 0.05 (OR=5.33
and RR=2.18), while extent of GM did not significantly differ. Table 3.
Frequency of GM in DU patients did not statistically differ much
according to HP status (55.9% for HP positive and 72.7%,
for
HP negative patients), p > 0.05. Also, an average score values
of GM did not statistically differ much according to HP status.
Table 4.
An analysis of the prevalence and extent of duodenal bulb GM in comparison
to the density of astral HP colonization in DU patients demonstrated
that the frequency of GM did not statistically differ much according to
the degrees of density of astral HP colonization. An average score
values of GM did not statistically differ much according to the degrees
of density of HP colonization. Table 5.
In the control group frequency of GM was not statistically much different according to HP status (25%, for HP positive and 33.3%, for HP negative patients), p > 0.05. Also, the average score values of GM did not statistically differ much according to HP status. Table 6.
Using the biopsy rapid urease test and histologic examination HE and Giemsa method, HP was not detected in the duodenal bulb in any case.
Duodenal gastric metaplasia (GM) is occasionally encountered histological change, which is traditionally relied on gastric hypersecretory status and subsequent duodenal mucosal chemical injury (9). When occurs, GM is unevenly distributed with the utmost spread within the bulb. If more extended there, GM can be tracked aboraly into the descending duodenum (6). The relationship between duodenal GM, gastric HP colonisation rate, and HCL secretory status seems to important to study in exploring DU pathogenesis (9). It is considered that in the presence of GM, HP may become a pathogenic agent for the occurrence of DU (8). It has been therefore accepted that the presence of HP in the duodenum, which colonises areas of GM, is important for DU pathogenesis (27).
There are several well-documented reports about the prevalence of GM in DU. According to Harris, GM is more frequent in DU (89%) than in non-ulcer patients (56%) (10). Other authors also found greater prevalence and higher extent of GM in DU (60-100%) than in controls (4-64%) (11-15). These variations may be the result of different number of performed duodenal biopsies. When smaller number of biopsies is made, there is greater probability of missing GM due to its uneven distribution. Therefore, at least two duodenal mucosal biopsies from both anterior and posterior wall for histology are recommended (6). Biopsies from the anterior wall of the duodenal bulb are particularly important, because GM is more frequent at that preferred site (6). Some authors recommend even greater number of biopsies from all quadrants of the bulb. Yang and associates found GM in 83% patients with DU when studied four biopsies from ulcer margins (16). By staining the duodenal bulb with methylen-blue during endoscopy, the possibility of detection of GM is increased. Noshiro and Mertz demonstrated that unstained areas in the bulb had significantly greater presence and extent of GM than stained ones (17,18). In our series, we confirmed that the prevalence of GM was significantly greater in DU patients, irrespectively to HP status. We found that the extent of GM was significantly higher in HP positive patients with DU than in the control group of HP positive non-ulcer patients
It is believed that GM occurs as a protective defense/ repair mechanism of the duodenal mucosa made by gastric acid damage. It is considered that there is a certain threshold of gastric acid secretion for GM occurrence (21). According to Harris there is direct positive correlation between the extent of duodenal GM and gastric acid secretion rate. The extent of GM was larger in individuals with greater basal and stimulated gastric acid secretion (10). The presence of higher level of gastric acid secretion in patients with DU, in comparison with healthy individuals, might explain the contribution of acidity in greater presence of GM in patients with DU (22, 23). However, GM is present in 22-64% of healthy individuals, who are not hypersecretors, as well as in a large percentage of patients with functional dyspepsia, which basal acid secretion is identical with healthy individuals, and whose circadian gastric acidity is lower than acidity in healthy individuals (13). These data show that the occurrence of GM is probably an answer to different factors that damages duodenal mucosa, including those associated with acid secretion. It is possible that rapid gastric emptying characteristic for DU may have part in the occurrence of GM and DU, as well as the inability to neutralise acid in duodenum with bicarbonates secreted by pancreas or duodenal mucosa (24). Further on, lower duodenal mucosal prostaglandin synthesis on graded and comparable decrease of duodenal pH in some DU and non-ulcer individuals is possibly another cause of duodenal mucosal damage and GM as cheap and quick repair mechanism in normal HCL secretor cases. This is further supported by the observation of the lack of influence of prolonged anti-secretory drugs treatment, such as H2 blockers, on the extent of GM, as well as the contradictory data on reversion of GM after vagotomy (24).
Many groups study the prevalence of GM according to HP status
in DU. Most authors were unable to rely the prevalence and extent of GM
with HP status (10,11, 13). According to Neri, the prevalence of
duodenal GM cannot be correlated with gastric antral HP colonisation
density rate (19). Wyatt did not find significant difference
in the prevalence of GM according to HP status (34% Vs 32%),
but when GM was present, it was more extensive in HP positive patients
(9). Oppositely Górnicka reported positive correlation
between antral HP colonisation density and prevalence of GM in the
duodenan bulb (20). In our study the prevalence and extent of duodenal
bulb GM did not statistically differ according to gastric HP status.
We found that in DU patients the prevalence and extent of duodenal bulb
GM did not statistically differ much according to the degrees of density
of
HP colonisation in the stomach antrum. Thus HP
infection was neither an obligatory factor for GM, nor the factor of extension
of already present GM (10, 11, 13, 19). In our patients, using rapid urease
test and mucosal histology with hematoxylin-eosin and Giemsa staining methods,
we did not verify the presence of
HP in the duodenum. This is possibly due to small
number of HP and sampling error because of uneven distribution of
GM, so that HP is rarely detected even in the cases
of greater extent of GM (27).
Using the quantitative cultivation method, HP is detected more frequently in duodenum. Hamlet reported HP positivity in 95% DU and in 80% of asymptomatic patients. Both groups had positive HP serology and positive HP in the stomach by the cultivation. Further on, both groups had similar density and proportional ratio of cagA positive breeds of HP in the antrum (86% and 75%, respectively), but DU cases had 20 times higher HP density and larger percentage of cagA positive strains in duodenum than asymptomatic patients (81% and 30%, respectively). The same author reported high density of cagA positive strains of HP in the duodenum with associated severe duodenitis and metaplastic mucosal milieu what he considered an important factor for DU pathogenesis (27).
The latest studies showed that the same person may have different strain of HP in the stomach antrum and duodenum according to their genotype and phenotype. Thoreson isolated in the same DU patients strains of HP with different characteristics according to their DNA profile and the expression of Lewis antigen, in the antrum and areas of GM in the duodenum. This is to suggest the complexity of interaction between HP and the host. It is possible that certain strains of HP may survive struggling to colonise the areas of GM in the duodenum, overwhelming older breeds and, finally, in the areas of GM, this leading to the occurrence of DU (28).
GM can be found in other parts of gastrointestinal tract, such as
the small intestine, rectum, gall bladder, pancreas, etc., in the presence
of chronic inflammation, such as Crohn’s disease, intestinal
tuberculosis etc. Because of that, it is not possible to exclude the role
of inflammation in the occurrence of GM, especially because there is no
acid in these parts of the digestive tract as a possible reason for the
occurrence of GM (24).
REFERENCES
Liu KC, Wright NA.The migration pathway of epithelial cells
on human duodenal villi: the origin and fate of gastric metaplastic cells
in duodenal mucosa. Epith Cell Biol 1992; 1: 53-8.
Shaoul R, Marcon P, Okada Y, Cutz E, Forstner G. The pathogenesis
of duodenal gastric metaplasia: the role of local goblet cell transformation.
Gut 2000; 30: 397-403.
Kühl P, Baczako K, Nilius M, Malfertheiner P.How does
gastric metaplasia in the duodenum differ from gastric epithelium? Gut
1995; 37 (Suppl 1): A29.
Wright NA. Is gastric metaplasia in Helicobacter
pylori really gastric? In: Hunt RH and Tytgat GNJ. Helicobacter
pylori – basic mechanisms to clinical cure 2000. Dordrecht.
Kluwer Academic 2000: 307-11.
Kushima R, Manabe R, Hattori T, Burckard F. Histogenesis
of gastric foveolar metaplasia following duodenal ulcer: a definite reparative
lineage of Brunner’s glands. Histopathology 1999; 35: 38-43.
Walker MM, Dixon MF.Gastric metaplasia: its role in duodenal
ulceration. Aliment Pharmacol Ther 1996; 10 (Suppl 1): 119-28.
Tovey FI, Hobsley M.Is Helicobacter pylori the primary
cause of duodenal ulceration?
J Gastroenterol Hepatol 1999; 14: 1053-6.
Talamini G, Zamboni G, Cavallini G.Antral mucosal Helicobacter
pylori infection density as a risk factor of duodenal ulcer. Digestion
1997; 58: 211-7.
Kokai G, Perisic VN. Sarjanovic Lj. Duodenalna gastricna metaplazija: veza izmedju aciditeta i Helicobacter pylori infekcije u dece sa duodenalnim ulkusom. Gastroenterohepatoloski arhiv 1991; 10: 42–3.
Wyatt JI, Rathbone BJ, Sobala GM, et al.Gastric epithelium
in the duodenum: its association with Helicobacter pylori and inflammation.
J Clin Pathol 1990; 43: 981-6.
Harris AW, Gummett PA, Walker MM, Misiewicz JJ, Baron JH.Relation between gastric acid output, Helicobacter pylori, and gastric metaplasia in the duodenum. Gut 1996; 39: 513-20.
Bago J, Kranjec D, Strini? D. Relationship of gastric
metaplasia and age, sex, smoking and Helicobacter pylori infection
in patients with duodenal ulcer and duodenitis. Coll Antropol 2000; 24:
157-65.
Uygun A, Kadayifci A, Demiriz M, et al.The effect of Helicobacter
pylori eradication on duodenal gastric metaplasia. J Int Med Res 1999;
27: 159-66.
Noach LA, Rolf TM, Bosma NB, et al.Gastric metaplasia and
Helicobacter
pylori infection. Gut 1993; 34: 1510-4.
Biad A, Hamladji RM, Bouhadef A.Gastric metaplasia in normal
man and patient with duodenal ulcer disease. Gut 1994; 35 (Suppl 4): A131.
Shabib S, Cutz E, Drumm B, Sherman P.Helicobacter pylori infection
is associated with gastric metaplasia in the duodenum. Gastroenterology
1992; 102: A163.
Yang H, Dixon MF, Zuo J, et al.Helicobacter pylori infection and gastric metaplasia in the duodenum in China. J Clin Gastroenterol 1995; 20: 110-2.
Noshiro M, Kusugami K, Sakai T, et al.Gastric metaplasia in
the duodenal bulb shows increased mucosal interleukin-8 activity in Helicobacter
pylori-positive duodenal ulcer patients. Scand J Gastroenterol 2000;
35: 482-9.
Mertz H, Kovacs T, Throson M, Weinstein W.Gastric metaplasia
of the duodenum: identification by an endoscopic selective mucosal staining
technique. Gastrointest Endosc 1998; 48: 32-8.
Neri M, Artese L, Pesa O, et al.Duodenal gastric metaplasia
and Helicobacter pylori infection: a cross-sectional study on 196
consecutive dyspeptic patients. IXth EHPSG International Conference 1996;
Abstracts-On-Disk®.
Górnicka B, Muszynski J, Bogdanska M. Gastric
metaplasia in duodenal bulb: correlation with Helicobacter pylori
infection and ulcer disease. 6th UEGW, Birmingham 1997; Gut
1997; 41 (Suppl 3): P697.
Dixon MF, Lee A and Veldhuyzen van Zanten SJO.Peptic ulcer
disease – the transitional zones are important. In: Hunt RH,
Tytgat GNJ. Helicobacter pylori – basic mechanisms to clinical
cure 2000. Dordrecht. Kluwer Academic 2000: 327-38.
Wagner S, Gladziwa U, Haruma K, Verrentrapp M, Gebel M.Effect
of Helicobacter pylori infection on 24 hour intragastric acidity
in patients with gastritis and duodenal ulcer. Gut 1992; 33: 1024-8.
Savarino V, Mela GS, Zentilin P, et al.Circadian acidity pattern
in prepyloric ulcers: a comparison with normal subjects and duodenal ulcer
patients. Scand J Gastroenterol 1993; 28: 772-6.
Savarino V, Mela GS, Zentilin P, et al.Circadian gastric acidity
in Helicobacter pylori positive ulcer patients with and without
gastric metaplasia in the duodenum. Gut 1996; 39: 508-12.
Fitzgibbons PL, Dooley CP, Cohen H, Appleman MD.Prevalence
of gastric metaplasia, inflammation, and Campylobacter pylori in the duodenum
of members of a normal population. Am J Clin Pathol 1988; 90: 711-4.
Khulusi S, Mendall MA, Badve S, Patel P, Finlayson C, Northfield
TC.Effect of Helicobacter pylori eradication on gastric metaplasia
of the duodenum. Gut 1995; 36: 193-7.
Hamlet A, Thoreson A-CE, Nilsson O, Svennerholm A-M, and Olbe
L. Duodenal Helicobacter pylori infection differ in cagA
genotype between asymptomatic subjects and patients with duodenal ulcers.
Gastroenterology 1999; 116: 259-68.
Thoreson A-CE, Hosseini N, Svennerholm A-M, and Bölin I.Different Helicobacter pylori strains colonize the antral and duodenal mucosa of duodenal ulcer patients. Helicobacter 2000; 5: 69-78.
|
|
|
|
|
| Patients (no) |
|
|
|
| Male/female (no) |
|
|
|
| Age (± SD) |
|
|
|
| Smokers/non-smokers (no) |
|
|
|
NS, not significant; * Mantel-Haenszel chi-squares test with Yates
corrected; ** Mann-Whitney U - Wilcoxon Rank Sum W test.
Table 2. Prevalence and extent of gastric metaplasia in the duodenal
bulb of H. pylori positive patients
| Group of patients |
Prevalence
of GM
Extent of GM
no (%)
score (1-4), ± SD |
|
| DU group (no=59) |
|
|
| Control group (no=28) |
|
|
| P values Odds ratio (95% CI) Relative risk (95% CI) |
3.81 (1.28-11.72) 2.24 (1.13-4.42) |
|
* Mantel-Haenszel chi-squares test with Yates corrected; ** Student’s
t test .
Table 3. Prevalence and extent of gastric metaplasia in the duodenal
bulb of H. pylori negative patients
| Group of patients |
Prevalence
of GM
Extent of GM
no (%)
score (1-4), ± SD |
|
| DU group (no=11) |
|
|
| Control group (no=27) |
|
|
| P values Odds ratio (95% CI) Relative risk (95% CI) |
5.33 (0.93-34.15)
|
|
NS, not significant; * Fisher’s exact test; ** Student’s
t test.
Table 4. Prevalence and extent of gastric metaplasia according to
H.
pylori status in the stomach in the DU group of patients
| H. pyloristatus |
Prevalence
of GM
Extent of GM
no (%)
score (1-4), ± SD |
|
| H. pyloripositive (no=59 ) |
|
|
| H. pylorinegative (no=11) |
|
|
| P values Odds ratio (95% CI) Relative risk (95% CI) |
0.48 (0.09-2.27) 0.77 (0.50-1.18) |
|
NS, not significant; * Fisher’s exact test; ** Student’s
t test.
Table 5. Prevalence and extent of gastric metaplasia in relation
to the density of H. pylori colonisation in the stomach antrum in
the DU group of patients (59 H. pylori positive)
| Degree of density of H. pylori colo-nisation in
the stomach antrum |
Prevalence of GM
Extent of GM
no (%)
score (1-4), ± SD |
|
| 1+ (no=17) |
|
|
| 2+ (no=q32) |
|
|
| 3+ (no=10) |
|
|
| P1-P3 values |
|
|
P1, 1+ density to 2+ density; P2, 1+ to 3+; P3, 2+ to 3+; NS, not significant; * Mantel-Haenszel chi-squares test with Yates corrected / Fisher’s exact test; ** Student’s t test.
Table 6. Prevalence and extent of gastric metaplasia in the control
group of patients according to H. pylori status in the stomach
| H. pyloristatus |
Prevalence of GM
Extent of GM
no (%)
score (1-4), ± SD |
|
| H. pyloripositive (no=28) |
|
|
| H. pylorinegative (no=27) |
|
|
| P values Odds ratio (95% CI) Relative risk (95% CI) |
0.67 (0.18-2.49) 0.75 (0.33-1.73) |
|
NS, not significant; * Mantel-Haenszel chi-squares test with Yates
corrected; ** Student’s t test.
Figure 1. Chronic duodenitis with extensive gastric metaplasia (
HE x 250).
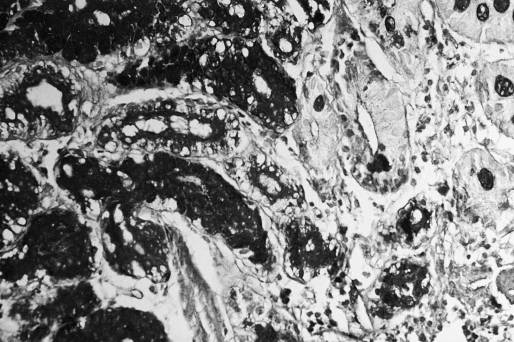
Figure 2. Chronic duodenitis and the focuses of gastric metaplasia
with apical PAS positive fucomucines in the cytoplasm of epithelial cells
( AB - PAS x 250 ).