Jetra i bilijarni trakt
ARCH GASTEROENTEROHEPATOL 2001; 20 ( No 3 - 4 ):
Case report
Suppurative cholangitis and cholestasis caused by infected congenital
liver cyst perforated into the left hepatic duct
Gnojni holangitis i holestaza prouzrokovani inficiranom kongenitalnom
cistom jetre perforiranom u levi duktus hepatikus
Radoje Colovic, Mirjana Perisic- Savic and Nikica Grubor
Institute of Digestive Diseases, Clinical Centre of Serbia, Belgrade.
Address correspondence to: Professor Dr Radoje Colovic
Institut of Digestive Diseases. Clinical Centre of Serbia,
Kosta Todorovica 6 Str,
YU-11000 Belgrade, Serbia, Yugoslavia
Tel.
+ 381 11 361 0 715/ Ext.133.
………………………… ……………………………
Suppurative cholangitis caused by infected liver cyst Gastroenteroloska Sekcija SLD-
01720, 2002.
SUMMARY
Congenital liver cysts are usually asymptomatic or accompanied by
abdominal discomfort. Although rare, they may cause variety of complications.
Infection of the cyst is, however, a very rare. We present a case history
of 40-year old man with congenital central liver cyst accidentally found
by ultrasonography. Two months later infection and perforation of the cyst
into left hepatic duct occurred, causing suppurative cholangitis, intensive
obstructive jaundice and mild pancreatitis. The patient was cured
by cholecystectomy,
T tube drainage of the common bile duct and by external drainage of the
infected cyst.
Key words: Congenital cyst, liver, infection, perforation, cholangitis,
jaundice, surgery.
SAZETAK
Kongenitalne ciste jetre su najcesce asimptomske ili prouzrokuju blage tegobe. Medjutim ponekada one mogu da prouzrokuju razlicite komplikacije. Infekcija ciste je jedna od njih. U radu se prikazuje slucaj pacijenta starog 40 godina kod koga je prethodno ultrazvucnim pregledom slucajno utvrdjena centralno polozena cista jetre. Dva meseca docnije doslo je do zagnojavanja ciste, njene perforacije u levi duktus hepatikus, i sledstvenog supurativnog holangitisa, ikterusa, i blagog pankreatitisa. Pacijent je izlecen holecistektomijom, drenazom duktus holedohusa T-drenom, i eksternom drenazom ciste.
Kljucne reci: Kongenitalne ciste, jetra, infekcija, perforacija, holangitis, ikterus, hirurgija.
INTRODUCTION
Congenital liver cysts are uncommon disorder. Several hundreds cases are already reported in the literature (1,2,3,4). However, widespread use of the new imaging techniques, ultrasonography (US) and computed tomography (CT) increase number of diagnosed liver cysts, particularly small ones. They are usually solitary, <10 cm in diameter, and rarely multiple (4.5,6). Females are more frequently affected (5). Right liver lobe is more oftenly involved (7). Renal cysts are associated in about 25% of cases, while splenic cysts are rare (8). Small liver cysts are usually asymptomatic. When present, symptoms are non-specific such as discomfort, abdominal distension, or mild pain probably due to compression of neighbouring organs. Cysts may be complicated by inartistic haemorrhage, spontaneous torsion of a pedicle, rupture into the abdominal cavity, malignant degeneration, portal hypertension, or may develop intracystic infection and obstructive jaundice (5,7,9,10-14,17,18-30).
CASE REPORT
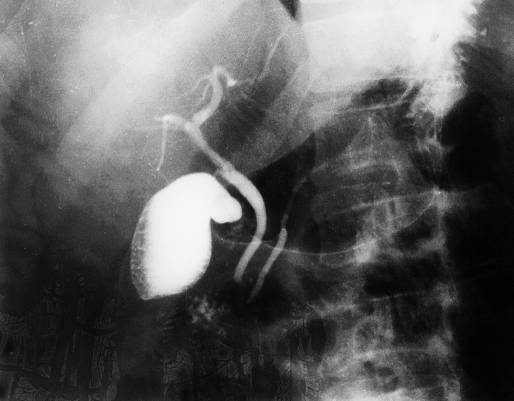
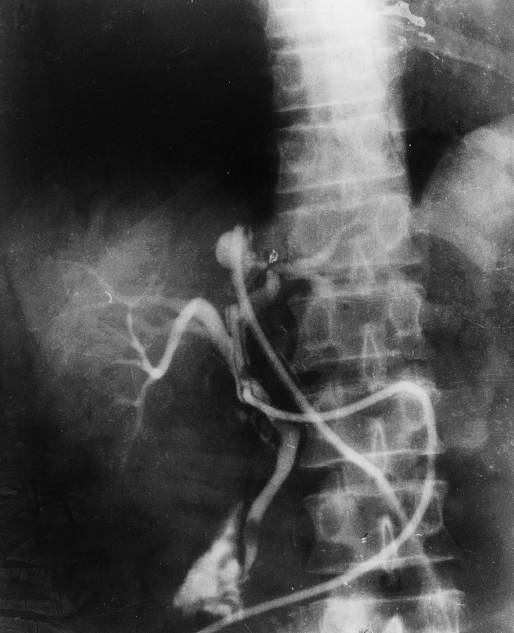
WE examined Forty years old man, because of urinary colic on 20.1.1989. A central liver cyst, 5x5 cm in diameter, just behind the liver hilus, was accidenty found. Figure 1. Intrahepatic bile ducts were slightly dilated. On 24.1.1989. ERCP was carried out, showing normal pancreatic and bile ducts, without any communication between liver cyst and bile ducts. Figure 2. Indirect immunofluorescence test for serum anti-echinococcus antibodies and indirect hemaglutination test were negative. Being asymptomatic, patient refused recommended operative treatment. Six weeks later fever, chills, right subcostal pain, and abdominal tenderness suddenly appeared. This was followed by progressive obstructive jaundice. Ultrasonography showed that liver cyst became more enlarged (diameter 7cm), bile ducts more dilated. A dense mass was seen in the common bile duct (CBD). On admission on 8.3.1989. the patient was jaundiced, with palpable, painful liver. Serum bilirubin was 142mmol/L, conjugated fraction 117mmol /L, alkaline phosphatase 4.8U/L (normal values 1-2.5 after Raabe). Serum transaminases, serum and urinary alpha-amylase were within normal limits. Despite parenterally given antimicrobials, the illness progressed so that the operation was performed on 15.3.89. Liver was enlarged, cholestatic, gallbladder appeared normal, CBD was 12 mm in diameter. Intraoperative cholangiography via cystic duct showed a communication between the left hepatic duct and centrally positioned hepatic cyst. Figure 3. Cyst was deeply located within the liver and therefore neither visible nor palpable. After choledochotomy a lot of turbid bile and pus from CBD and intrahepatic bile ducts was drained. Intestinal bacterial flora was isolated. Both instrumentally and choledochoscopicaly, communication between left hepatic duct and liver cyst was documented. Through hepatotomy on the lower surface of the segment IV, central liver cyst in the depth of 3 cm was found. Cystoscopy using fiberoptic choledochoscope demonstrated smooth and partly trabecular white-reddish internal surface and epithelial turbidity with spotty haemorrhages. No tumour or gallstone was seen. Since the cyst was inconvenient for omentoplasty, Foley’s catether of 24 F was inserted into the cystic cavity through hepatotomy, gallbladder was removed, and T-tube was placed into the CBD. This led to full recovery with gradual normalisation of laboratory data including serum bilirubin. Two weeks later, communication between cyst and left hepatic duct was closed; cyst gradually became smaller and finally disappeared. Figure 4. Then T-tube and Foley’s catether were removed and patient was discharged enjoying good health more then 11 years until now. Follow-up US and CT of the liver were normal.
Non-parasitic simple cyst of the liver long has been considered a rare lesion. In fact, symptomatic or complicated simple cyst are uncommon, but asymptomatic simple cyst are found in about 1% of adults at autopsy. They tend to be large in adults over 50 than in younger individuals. Rarely cyst grows rapidly, and this is observed exclusively in woman over 50. Complications are uncommon, the most frequent being intracystic bleeding. The clinical manifestation is sudden, severe pain, and increase in size of the cyst.
Infection of the liver cyst is poorly described complication. There
are very few well-documented cases of the infection of the liver cysts
in the literature. Most authors refer to the paper of Flagg and Robinson
1967 (7). In their series secondary infection of the solitary cysts were
recorded only in treated patients. Therefore our case represent a very
rare occasion of preoperative spontaneous infection of congenital liver
cyst, leading to perforation into bile ducts, suppurative cholangitis and
obstructive jaundice. Pathogenesis of infection of liver cyst in our patient
is not clear. It could have been caused by ERCP, the only invasive diagnostics
we performed. However, ERCP was made 6 weeks before infection and in the
meantime the patient was symptom-free. Other cause of infection like stone
was not found.
Obstructive jaundice itself due to congenital liver cysts is another rare complication, compared to other hepatic space-occupying lesions of equal size. Simple cysts produce little inflammation and adhesions, without invasion of normal liver tissue. They only exert external compression, growing slowly with low internal tension. Pressure on surrounding liver tissue and bile ducts increases slowly. The cysts do not occlude bile ducts directly (29). Jaundice is usually mild and transitory due to intermittently increased pressure on bile ducts, probably due to intracystic haemorrhage.
Treatment of uncomplicated congenital liver cysts is necessary only in symptomatic and complicated cases or if cysts are of greater size. Operative methods are well established and depend on localisation and content of cyst (5,32). Prolonged external drainage of the infected cyst until it disappears was successfully performed in our patient. It was the simplest way of treatment for the cyst being central, deep inside the liver.
REFERENCES:
Jones WL, Mountain JC, Warren kW. Symptomatic non-parasitic cysts
of the liver. BJ Surgery 1974; 61:118-23.
Sanfelippo PM, Beahrs OH, Weiland LH. Cystic disease of the liver.
Ann Surg. 1974;179:922-5.
Williamson RCN, Ramus NI, Shorey BA. Congenital solitary cysts of the liver and spleen. Br J Surg 1978;65:671-3.
Rashed A, May RE, Williamson RCN. The management of large congenital
liver cysts. Postgrad Med J 1982;58:536-41.
Hadad AR, Westbrook KC, Graham GG, Morris WD, Campbell GS. Symptomatic non-parasitic liver cysts. Am J Surg 1977;134:739-44.
Davis CR. Liver cysts, non parasitic. Crace Hosp. Bull. ( Detroit)
936;20:2-48.
Flagg RS, Robinson DW. Solitary nonparasitic hepatic cysts: report
of oldest known case and review of the literature. Arch Surg 1967; 95:664-73.
Henson SW Jr, Gray HK, Dockerty MB. Benign tumors of the liver IV.
Polycystic disease of surgical significance. Surg Gynecol Obstet 1957;
104:63-7.
Grime RT, Moore T, Nicholson A, Whitehead R. Cystic hamartomas and
polycistic diseases of the liver. Br J Surg 1959;47:307-13.
Orr TG, Thurstone JA. Strangulated non parasitic cyst of the liver.
Ann Surg 1927;86:901-4.
Cruickshank AH, Sparshott SM. Malignancy in natural and experimental
hepatic cysts: experiments with alfatoxin in rats and the malignant transformation
of cysts in human livers. J Pathol 1971;104:185-90.
Sood SC, Watson A. Solitary cyst of the liver presenting as an abdominal
emergency. Postgrad Med J 1974; 50:48-50
Morgenstern L. Rupture of solitary non-parasitic cysts of the liver.
Ann Surg 1959; 150:167-71.
Horton RE. Giant cyst of the liver complicated by rupture. Br J Surg
1954;41:442-4.
Richmond HG. Carcinoma arising in congenital cysts of the liver. J Path Bact 1956; 72:681-3.
Ratcliffe PJ, Reeders S, Theaker JM. Bleeding esophageal varices
and hepatic disfunction in adult polycystic kidney disease. Br Med J 1984;288:1330-1.
Del Guercio E, Greco J, Kim KE et al. Esophageal varices in adult patients with polycystic kidneys and liver disease. N Engl J Med. 1973;289:678-9.
Wittig JH, Burns R, Longmire WP Jr. Jaundice associated with polycystic
liver disease. Am J Surg 1978;136:383-6.
Clinckscales NB, Trigg LP, Poklepovic J. Obstructive jaundice secondary
to benign hepatic cyst. Radiology 1985;154:643-4.
Fernandez M, Cacioppo JC, Davis RP et al. Management of solitary
nonparasitic liver cyst. Am Surg 1984;50:205-8.
Ergun H, Wolf BH, Hissong SL. Obstructive jaundice caused by polycistic
liver disease. Radiology 1980;136:435-6.
Morin ME, Baker DA, Vanagunas A, Tan A, Sue HK. Solitary non-parasitic
hepatic cyst causing obstructive jaundice. Am J Gastroenterol 1980; 73:434-6.
Machell RJ, Calne RY. Case report: solitary non parasitic hepatic
cyst presenting with jaundice. Br J Radiol. 1978;51:631-2.
Santman FW, LG Thijs LG, Van der Veen EA, Den Otter G, Blok P. Intermittent
jaundice: a rare complication of a solitary nonparasitic liver cyst. Gastroenterology
1977;72:325-8.
Howard RJ, Hanson RF, Delaney JP. Jaundice associated with polycistic
liver disease: relief by surgical decompression of the cysts. Arch Surg
1976;111:816-7.
Sacks HJ, Robbins LS. Fistulization of a solitary hepatic cyst. JAMA 1967;200:415-7.
Dardik H, Glotzer P, Silver C. Congenital hepatic cyst causing jaundice.
Ann Surg 1964;159:585-2.
Hudson EK. Obstructive jaundice from solitary hepatic cyst. Am J Gastroenterol 1963;39:161-4.
Cappell MS. Obstructive jaundice for benign nonparasitic hepatic cysts: identification of risk factors and percutaneous aspiration aspiration for diagnosis and treatment. Am J Gastroenterol 1988; 83:93-6.
Colovic R, Colovic M, Perisic-Savic M, Krivokapic Z. Kongenitalne
ciste jetre. Prikaz cetiri bolesnika i pregled literature. Gastroenterohepatol
Arch 1988; 7:96-100.
Grunfeld JP, Albouze G, Jungers P et al. Liver changes and complications in adult polycistic kidney disease. Adv Nephrol 1985; 14:1-20.
Longmire WP. Jr, Tompkins RK. Mannual of Liver Surgery. New York-Heidelberg:
Springer Verlag, 1981.
Figures: