Gastroenterohepatologic iconography
Gastroenterohepatoloska ikonografija
ARCH GASTROENTEROHEPATOL 2000; 19 ( No 3 – 4 ):
Blood dyscrasia caused by wandering spleen reversed by partial splenic resection and splenopexy.
Hematoloski poremecaji prouzrokovani lutajucom slezinom koji su korigovani delimicnom resekcijom slezine i splenopeksijom.
Surgery of wanedring spleen
( accepted November 21st, 2000 )
1Bozina Radevic, 2Dragan Sagic, 3Vojislav N. Perisic,3Mira Petrovic
1Surgical Clinic, Institute for Cardiovascular Diseases Dedinje, 2Department of Radiology, Institute for Cardiovascular Diseases Dedinje, 3University Children , s Hospital, Belgrade.
Address correspondence to: Professor Dr VN.Perisic
University Children , Hospital
10 Tirsova St.
YU-11000 Belgrade, Serbia,
Yugoslavia
E-mail:[email protected]
An 11-year old by was referred for further evaluation of his dull abdominal pain of lesser degree and haematological abnormalities ( anemia, leukopenia, and trombocytopenia ). He was previously hospitalised at the Institute of Mother and Child, N.Belgrade without definite diagnosis and recommended treatment.
At admission central abdominal mass and “ empty “ left hypochondrium were felt by palpation. Immediate abdominal ultrasound scan examination with Doppler technique showed that abdominal tumour is enormously enlarged wandering ( ectopic ) spleen with normal arterial perfusion and venous drainage. Laboratory investigations demonstrated haematological abnormalities of hypersplenism ( anemia, leukopenia, trombocytopenia ) and normal liver function tests.
Superior mesenteric arteriography showed partially reversed flow via pancreatico-duodenal arcades and and gastroduodenal artery to the hepatic and the lienal artery ( hepatolienal steal). Figure 1.
Lienal artery angiography confirm the presumptive diagnosis of wandering spleen which sized the pelvic floor. Figure 2.
Splenic lower lobe resection and splenopexy below the left diaphragm dome was performed successfully without interfering splenic arterial and venous blood flow at the Institute for cardiovascular diseases Dedinje by one of us ( BR ). Postoperative course was uneventful. After operation quick and full haematological recovery occurred with normalization of leukocyte and trombocyte count.
Follow-up angiography of splenic artery demonstrated spleen “ in situ “ ( left hypochondrium ) with reduced parenchymal mass. Figure 3a&b. Superior mesenteric angiography showed drastically reduced retrograde flow toward hepatic artery ( hepatic steal ) without splenic phase. Figure 4.
Comment: Management recommendations to treat wandering spleen have varied, but recognition of significant number of postsplenectomy sepsis supports splenic preservation approach. It is stated that splenectomy is only reserved for patients presenting with acute abdomen due to splenic infarction or thrombosis or with hyperspenism and in patients in whom splenopexy is technically unfeasible ( 1 ). Splenic detorsion combined with splenopexy may be considered a reasonable surgical option even in patients with acute abdomen, if there is no evidence of splenic infarction, splenic vein thrombosis, and hypersplenismus ( 2 ). Laparoscopic splenopexy seems to be effective procedure for wandering spleen with the advantage of minimally invasive surgery ( 3,4 ).
There are two reports about surgical management of wandering spleen from Serbian surgical centers quoted in Pub Med ( 5,6 ). In the first, Popovic M et al presented their experience with 2 adult cases with intermittent abdominal pain due to wandering spleen. They preferred splenectomy as treatment of choice ( 5 ). In the second report, Zivkovic SM reported his experience with paediatric ( infant ) cases with gastric volvulus combined with mobile spleen. He preferred sutureless “ button and hole “ splenopexy, which understands mobile spleen interposition between postero-lateral abdominal wall muscles and parietal peritoneum ( 6 ).
The management strategy of wandering spleen presenting with symptoms and signs of left-sided portal hypertension and splenomegaly combined with hypersplenismus is still controversial. In this cases in the majority of surgical centers splenectomy was advocated as treatment of choice ( 7,8 ). Subtotal splenectomy and splenic autotransplantation were considered to be of limited value ( 1 ). On the contrary our case further demonstrates the usefulness of subtotal splenic resection combined with splenopexy in paediatric cases at least. This approach reverses hematological abnormalities due to hypersplenism and prevents postsplenecomy sepsis.
In conclusion: to our best knowledge this is one of very few reported cases of partial splenic resection combined with splenopexy for wandering spleen associated with splenomegaly and hypersplenism. This approach is very important in paediatric patients in which the risk of postsplenectomy sepsis is high. Subtotal splenectomy fully reverse haematological abnormalities due to hypersplenism.
REFERENCES:
1.Buchner M, Baker MS. The wandering spleen. Sur Gynecol Obstet 1992; 175: 373-87.
2.Dawson JH, Roberts NG. Management of the wandering spleen. Aust NZJ Surg 1994; 64: 441-4.
3.Hirose R, Kitano S, Bando T, et al. Laparoscopic splenopexy for pediatric wandering spleen. J Pediatr Surg 1998; 33: 1571-3.
4.Cohen MS, Soper NJ, Underwood RA, Quaserbarth M, Brunt LM. Laparoscopic splenopexy for wandring spleen ( pelvic ) spleen. Surg Laparosc Endosco 1998; 8: 286-90.
5.Popovic M, Knezevic S, Colovic R, Petrovic M, Antunovic P, Djordjevic M. Ectopic spleen- 2 case reports. Acta Chir Iugosl 1995; 42: 59-62.
6.Zivkovic SM. Sutureless “ button and hole “ splenopexy. Pediatr Surg Int 1998; 13: 220-2.
7.Melikoglu M, Colak T, Kavasoglu T. Two unusual cases of wandering spleen requuuiring splenectomy. Eur J Pediatr Surg 1995; 5: 48-9.
8.Angeras U, Almskog B, Lukes P, Lundstam S, Wiess L. Acute gastric hemorrhage secondary to wandring spleen. Dis Dis Sci 1984; 29: 1159-63.
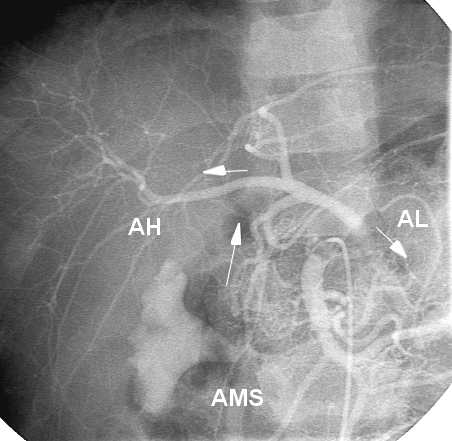
Figure 1. Superior mesenteric angiography Note hepato-lienal blood steal from the superior mesenteric artery ( AMS ) - reversed blood from from AMS via pancreatico-duodenal arcades ( arrow ) and gastroduodenal artery to common hepatic ( AH ) ( arrow ) and lienal artery ( AL ) ( arrow ).
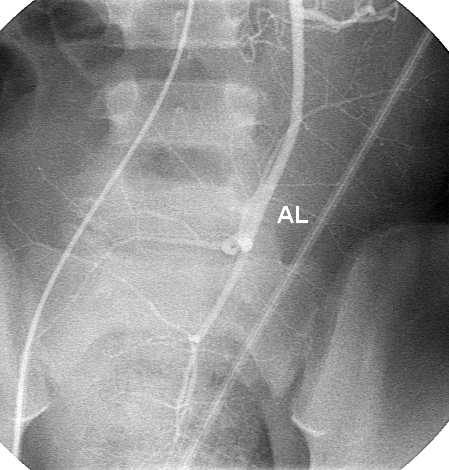
Figure 2. Lienal artery angiography Splenic artery ( AL ) is directed downward to the bottom of the pelvic floor. Lower splenic pole is seizing pelvis minor.
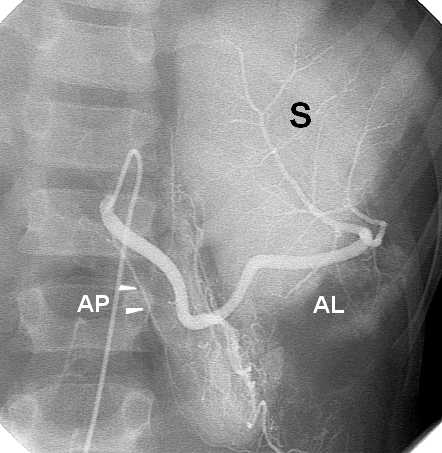
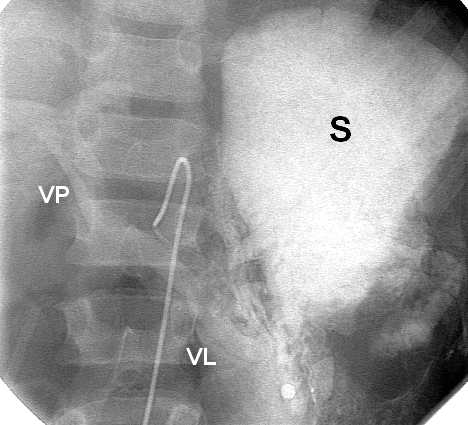
Figure 3. Postoperative lienal artery angiography 3a. Lienal artery ( AL ) is perfusing partialy resected spleen ( S ) located in the left hypochondrium. Pancreatic arcade is seen as well ( arrow ).
3b. Parenchymal phase. Note spleen in situ. Lienal vein ( VL ) and portal vein ( VP ) are demonstrated.
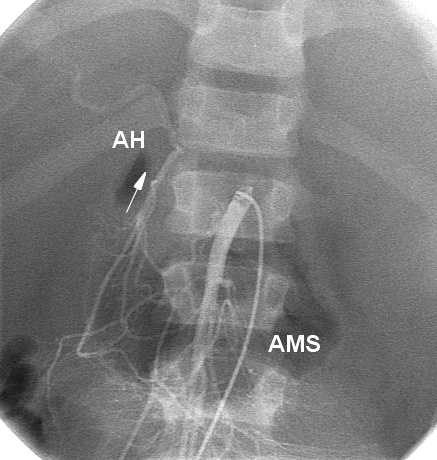
Figure 4. Postoperative superior mesenteric angiography There is drasticaly reduced retrograde flow from superior mesenteric artery ( AMS ) toward hepatic artery ( AH ) ( hepatic steal ) via pancreaticoduodenal arcades ( arrow ). There is no splenic phase.