Alimentary tract and pancreas
Alimentarni trakt i pankreas
ARCH GASTROENTEROHEPATOL 2000; 19 ( No 2 – 3 ):
PRIMARY MALIGNANT MESOTHELIOMA OF THE GREATER OMENTUM
Primarni maligni mezotelijom velikog opornjaka
Mesothelioma of the greater omentum
( accepted August 27th, 2000 )
1Charalambos Lazaridis, 1Basilios Papaziogas, 1Anastasios Souparis, 1Theodoros Pavlidis, 2Rodi Kotakidou, 2Georgios Paraskevas, 1Helena Argiriadou, 1Thomas Papaziogas.
1 2nd Surgical Clinic of the Aristoteles University of Thessaloniki, 2 Department of Pathology , G.GENNIMATAS Hospital, Greece.
Address correspondience to: Dr Basilios Papaziogas ,
Bl. Gabriilidi str. 29, 546 55 Thessaloniki, Greece
FAX : +30 31 99 25 63
E-mail : [email protected]
ABSTRACT
Peritoneal mesothelioma is a rare neoplasm and forms about 10% of all mesotheliomas. We report on a case of a primary malignant mesothelioma of the peritoneum of the greater omentum in a 83 year old male, who presented with ascites, weight loss, and symptomatic cholelithiasis. The diagnosis was set intraoperatively , with biopsy of the greater omentum. Due to the advanced spread of the tumor, the advanced age of the patient and his poor general condition, no additive therapy was applied. The patient underwent postoperatively multiple palliative paracentesis of the ascites, and finally died 12 months after the diagnosis.
Key words: malignant mesothelioma, peritoneum.
SAZETAK
Peritonealni mezotelijom je redak tumor koji prestavlja oko 10% svih mezotelijoma. U radu se prikazuje slučaj primarnog malignog mezotelijoma velikog opornjaka u muškarca zivotne dobi 83 godine, u koga se bolest ispoljila ascitesom, gubitkom telesne mase, i simptomima holelitijaze. Dijagnoza je postavljena u toku operativnog zahvata i potrdjena je hirurškom biopsijom velikog omentuma. Kako je tumor bio uznapredovao, i uzimajuci u obzir odmaklu dob i rdjavo opšte stanje bolesnika, nikakve dodatne mere lelenja nisu sprovedene. U postoperativnom toku radjene su ponavljane abdominalne paracenteze u cilju evakuacije ascitnog izliva. Do letalnog ishoda je došlo 12 meseci posle postavljanja dijagnoze.
Ključne reči: maligni mezotelijom, peritoneum.
INTRODUCTION
The mesothelioma of the peritoneum presents a malignant tumour of the mesothelomatous cells of the peritoneum. These tumours are similar to the mesotheliomas of the pleura. The causative relation with chronic exposure to asbestos, which is proved for mesotheliomas of the pleura has been confirmed also for the mesotheliomatous tumors of the abdominal cavity .( 1,2,3 ). Interestingly, peritoneal mesotheliomas are common in patients with heavy asbestos exposure, whereas pleural mesotheliomas predominate in the larger population of transiently exposed individuals ( 3 ).
The annual incidence of the tumour in the general population is 1-2 cases per million ( 4 ). It seems, that there is a gradual increase of the incidence of the tumour in the United States over the past decades ( 3 ).
The tumour usually affects older males, over 50 years of age. The symptomatology of the tumour is usually not specific, leading to a delay of the diagnosis ( 5 ).The patient usually presents with gradually developing ascites and weight loss, which in most of the cases indicates an intraperitoneal spread of the tumour.
The prognosis of malignant mesothelioma is relative poor.
CASE REPORT
A 83 year old male presented with a two months history of diffuse abdominal pain, and a weight loss of 5 kg. The patient complained about intermittent episodes of postprandial right subcostal pain, with radiation to the back, and nausea.
The ultrasonography of the upper abdomen revealed the presence of cholelithiasis, with signs of chronic cholecystitis, as well as ascitic fluid covering the surface of the liver. The laboratory findings were in the normal range except from a slightly increased serum amylase.
The computed tomography of the abdomen showed the presence of ascitic fluid, as well as a thickening of the greater omentum and the root of the mesentery. No enlarged intraperitoneal lymphnodes were noted. Figure .
The patient underwent exploratory laparotomy. After the opening of the peritoneum a large quantity of ascitic serosanginous fluid was aspirated, and sent for cytological examination. The greater omentum showed a diffuse infiltration. A typical omentectmy was performed. The exploration of the abdominal cavity revealed the presence of diffuse whitish metastatic spots on the serosa of the ileum and a thickening of the mesentery of the terminal ileum. The palpatory control of the colon, pancreas, stomach and liver was negative for the presence of suspect lesions.
The postoperative course of the patient was completely uneventful, and he was discharged from the clinic the 7th postoperative day.
The cytological examination of the ascitic fluid showed the presence of multiple atypical mesotheliomatous cells.
The biopsy showed the presence of a diffuse infiltration of the omentum and its surface with malignant mesotheliomatous cells, and multiple psamomma bodies. Figure 2.
Due to the advanced spread of the tumour, the advanced age of the patient and his poor general condition, no additive therapy was applied. The patient underwent postoperatively multiple palliative evacuating punctures of the ascites, and finally died 12 months after the diagnosis.
DISCUSSION
The mesothelioma of the peritoneum presents an extremely rare malignancy of the abdominal cavity. Most cases occur in patients over 40 years of age, but it has been also described in young adults, children and neonates ( 6 ). A significant predisposition of males for the development of this tumour has been noted .( 7,8 ).
About half of the cases seem to be associated with chronic heavy exposure to asbestos, with a latency period of approximately 15 years. The exposure to Thorotrast has also been implicated as a possible causative factor ( 3,9,10 ).
A malignant mesothelioma can rise from any serous surface of the body. The coexistence of malignant peritoneal and pleural mesotheliomas has also been described, and is usually associated with heavy chronic asbestos exposure. Ascoli et al described a case of concominant malignant mesothelioma of the pleura, peritoneum and tunica vaginalis testis ( 13 ). An extension to the retroperitoneal space is extremely rare but possible ( 14 ).
The patients present typically with recurrent ascites, abdominal cramps and gradually increasing abdominal girth. Partial bowel obstruction can also occur. However, the symptomatology of the tumour is usually not specific, leading to a delay of the diagnosis and possible effective treatment of the tumour ( 4,7,11,15,16 ). In some instances, the tumour can be manifested in the umbilicus. Rarely, the metastatic inguinal or cervical lymphnodes can be the first sign of the tumour ( 3,17 ).
The ultrasonography or CT of the abdomen usually confirm only the presence of ascites, or exclude the presence of other intrabdominal malignancy. The use of cytology after aspiration of the ascitic fluid can lead to the diagnosis, although the method cannot always distinguish malignant mesothelioma from metastatic carcinoma ( 18 ). The use of diagnostic laparoscopy, when performed, permits the direct biopsy of the tumour ( 4 ).
In general, peritoneal mesothelioma usually appears as multiple plaques or nodules scattered over the visceral or parietal peritoneum. Dense intraperitoneal adhesions, fibrous plaques or shortening of the mesentery can also be present. In advanced stages the peritoneal cavity can be completely obliterated by the tumour. Rarely, the tumour can present as an isolated mass, which has to be distinguished from benign mesothelioma ( 3 ).
The microscopic pattern of malignant mesothelioma is highly variable. The most common appearance is that of papillae or tubules lined by atypical mesothelial cells. Psammoma bodies or sarcomatoid spindle cells can also be observed. The mesothelial cells are usually acidophilic or vacuolated with large vesicular or hyperchromatic nuclei. In other instances, the cells may appear foamy as a result of lipid accumulation or can develop hydropic changes. Cartilagous or other types of mesenchymal metaplasia are also common.
Extracellular mucosubstances are often present, usually in the form of mucopolysaccharides. Immunocytochemically, the cells of malignant mesotheliomas are strongly positive for keratine, epithelial membrane antigen, and basement membrane-related proteins, and are generally negative for CEA and Leu-M1( 3 ).
The main differential diagnosis of malignant mesothelioma are the reactive mesothelial hyperplasia and the presence of metastatic carcinoma, particularly of the serous papillary type. (18)
The prognosis of the malignant peritoneal mesothelioma is extremely poor. Most patients die of the disease within 2 years of the diagnosis. Some encouraging results are reported with a combination of surgical debulking operations and intraperitoneal or systematic chemotherapy ( 19,20 ).
Surgery aims at achieving complete or near–complete cytoreduction of the tumour , usually with debulking procedures. The use of intraperitoneal chemotherapy can reduce the mass of the tumour and the ascites with less systemic toxicity. The use of cisplatin and mitomycin or anthracyclin have been proposed ( 21,22 ).
REFERENCES:
Fontana A., Fuchs P., Otto R.: „Malignant peritoneal mesothelioma.” Schweiz Med Wochenschr 1976 , 106(16) : 555-558.
Giles TD., Henderson JC., Dominguez GH.: “Diffuse malignant mesothelioma of the peritoneum.” South Med J 1967 , 60(1) : 53-66.
Chapter 26: Peritoneum, retroperitoneum and related structures” in Ackerman’s Surgical Pathology ,1992, p. 2143-2146.
Catania V., Bonaccorso R., Fraggetta F., Vecchio S., Grasso F., Cammisuli F., Minutolo V., Cavallaro V.: “Peritoneal mesothelioma.A case report.” Ann Ital Chir 1996 , 67(5) : 697-701.
Shimoyama S., Konishi T., Kawahara M., Araki S., Hojo K., Hamakawa S., Nagayama T. : “A rare case of primary mesothelioma originating from the rectovaginal tissue.” Hepatogastroenterology 1998 , 45(23) : 1593-1597.
Mc Cullagh M., Keen C., Dykes E.: “Cystic mesothelioma of the peritoneum:a rare cause of ascites in children.” J Pediatr Surg 1994 , 29(9) : 1205-1207.
Roggli VL., Oury TD., Moffat EJ.: “Malignant mesothelioma in women.” Anat Pathol 1997 , 2 : 147-163.
Fox H.: “Primary neoplasia of the female peritoneum.” Histopathology 1993 , 23(2) : 103-110.
Hausegger KW., Leither G.: „A malignant mesothelioma of the peritoneum following radiotherapy.A case report.” Radiologe 1992 , 32(4) : 170-173.
Horie A., Hiraoka K., Yamamoto O., Haratake J., Tsuchiya T., Sugimoto H.: “An autopsy case of peritoneal malignant mesothelioma in a radiation technologist.” Acta Pathol Jpn 1990 , 40(1) : 57-62.
Wouters EF., Havenith MG., Vermeulen A., Greve LH.: “Malignant mesothelioma presenting in the pleura and peritoneum.” West J Med 1984 , 27(6) : 213-217.
Mischler NE., Chuprevich T., Johnson RO., Tormey DC.: „Malignant mesothelioma presenting in the pleura and peritoneum.” J Surg Oncol 1979 . 11(3) : 185-191.
Ascoli V., Facciolo F., Rahimi S., Scalzo CC., Nardi F.: “Concominant malignant mesothelioma of the pleura, peritoneum, and tunica vaginalis testis.” Diagn Cytopathol 1996 , 14(3) : 243-248.
Iguchi Y., Toma H., Okumura T., Takahama M.: „Retroperitoneal malignant mesothelioma.A case report.” Nippon Hinyokika Gakkai Zasshi 1996 , 87(11) : 1261-1265.
Thankachan VA., Archana S., Kurien T., Ramakrisha B., walter D., Seshadri MS., Cherian AM.: “Malignant mesothelioma of peritoneum.A case report.” J Assoc Physicians India 1992 , 40(11) : 763-764.
Weidner N.: „Malignant mesothelioma of peritoneum.” Ultrastruct Pathol 1991 , 15 (4-5) : 515-520.
Hofner W., Potzi P., Feigl W., Schratter M.: „Mesothelioma of the peritoneum with pulmonary metastases.” Wien Med Wochenschr 1979 , 129(16) : 452-455.
Tauchi PS., Caraway N., Truong LD., Kaplan AL., Ramzy I.: “serous surface carcinoma of the peritoneum: useful role of cytology indifferential diagnosis and follow-up.” Acta Cytol 1996 , 40(3) 429-436.
Richter B., Richter P., Buchholz K.: „Malignant mesothelioma of the peritoneum . Case report“ Zentralbl Gynakol 1983 , 105(9) : 598-601.
Yamaguchi K., Naitoh S., Nomura S.: “A case of malignant mesothelioma of the pleura and the peritoneum detected by sudden onset of back pain and pleural effusion and ascites.” Nihon Kyobu Shikkan Gakkai Zasshi 1997 , 35(9) : 996-1002.
Tohda G., Kane T., Kosaka S., Takahashi T., Okuno T., Yamazaki T., Kanasaki S., Matsumoto K., Bamba T.: “A case of peritoneum malignant mesothelioma responding to arterial infusion chemotherapy” Nippon Shokakibyo Gakkai Zasshi 1997 , 94)6) : 445- 449.
Averbach AM., Sugarbaker PH.: “Peritoneal mesothelioma: treatment approach based on natural history.” Cancer Treat Res 1996 , 81 : 193-211.
FIGURES:

Figure 1. CT of the abdomen. Thickening of the greater omentum and the root of the mesentery.
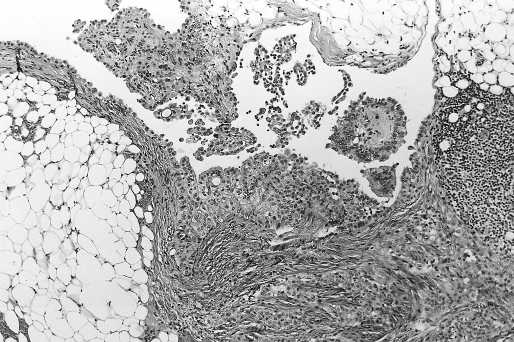
Figure 2. Tumour histology ( HE x 25 ) Infiltration of the omentum with malignant mesotheliomatous cells, which cover also the surface of the omentum. Multiple psamomma bodies are visible.
.