Health Economics and its Role in Health Sector Reform: Thai Experience
Dr. Siripen
Supakankunti
WHO Collaborating Centre for Health Economics
Faculty of Economics
Chulalongkorn University
Thailand
1. Thai Economy: Its Expansion and Contraction
Thailand’s economic structure is changing toward more industrialization and the Gross Domestic Product (GDP) increased about 7-9% annually from the late 1980s until 1996. The Thai economy took an unexpected downturn in 1996. The Bank of Thailand forecast the growth rate of Thai economy would expand at a rate of 2.0-3.0 percent only, caused by the poor performance of exports and private sector investment. Import growth also declined during 1996. Slowing the growth in imports alone cannot improve the country's current account deficit significantly. The deficit remains an economic problem of major concern. However, the economic stability believes to be improved as a result of harshness policies or expenditure cuts and savings acceleration. The budget deficit will be about 40,000 million baht.
2. Factors Determining Health
Health and Health Status are influenced by various factors namely the situations and trends of economic, social, political, administrative, physical environment, infrastructure development and technology development.
In sum, the economic growth and structure have made changes in the consumption pattern of Thai people. People need more health care and spend more for health services, both necessary and unnecessary care. The national health expenditure has been increasing gradually, at a rate faster than the Gross Domestic Product (GDP), from 3.5% of GDP in 1979 to 6.3% of GDP in 1991. In the year 2000 it’s expected to be at a rate of 8.1% of GDP. With the worst scenario of Thai economy it is expected to be more than 10% of GDP in future. The expenditure mostly covered by the household and the poor have a higher share of expenditure to income than the rich. The expense is for curative rather than preventive and promotive care. Moreover, the technologies for medical services are freely imported with some special tax exemption. This results in greater purchase and competition in importing the high cost equipment and unbalanced utilization of this equipment nation wide.
The Thai economic structure has changed from agriculture based industry to more manufacturing and service based industries. This caused people to move to industrially based areas or to migrate from rural to urban areas and society faces many social problems including occupational health. There is a great economic loss due to road accidents and accidents in the factory because of inadequate attention to industrial safety. The problem of air, water, noise and sight pollution in factory and environment and under standard working conditions is increasing. The increasing rate of using modern technology and chemicals in agricultural activities, i.e., pesticides, herbicides, artificial fertilizer has resulted in people receiving substances toxic to their health.
Income disparity between the poor and the rich, the rural and the urban areas, the agricultural and manufacturing sectors affect the health system in terms of inequity in health resource allocation. The free trade system also has impact on pharmaceutical industry: higher price of drugs because of the patent regulations.
Due to the problem of changes in education many people have limited abilities to adjust to the information received through the various media. Some change their health behaviour to adopt more risk to their health. There are also the problems of communicable diseases, chronic disease, elderly disease among the people.
3. Economic Crisis from mid 1997
The current economic crisis has enormous impact on the country and this impact will persist for at least 4-5 years. The immediate effects are unemployment, reduced household income and reduced consumption expenditure. These have social and health consequences.
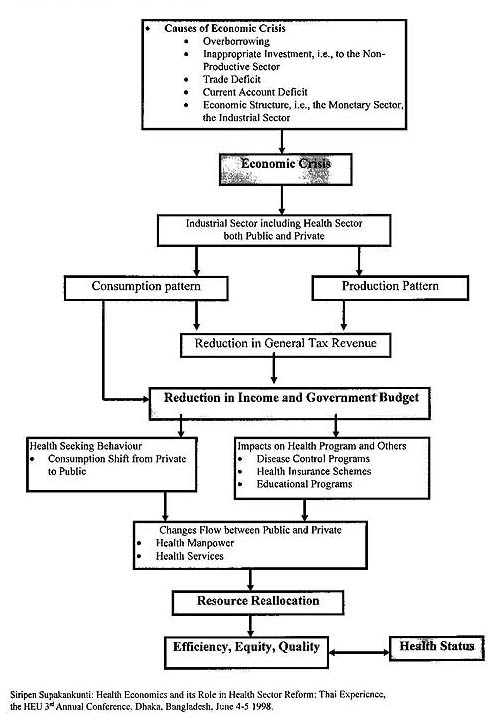
4. Economic Crisis and Health Impacts
5. Some Elements of Reforms in Health Sector
Soft loans from World Bank (WB) and Asian Development Bank (ADB) were offered to the Government to replenish the foreign reserves, and to support essential programs. These loans came with certain conditions to preserve the safety net to save the vulnerable groups, especially those unemployed. Under the recent loan from the Asian Development Bank (ADB), there are also elements of reforms in the health sector as conditions of the loan, namely
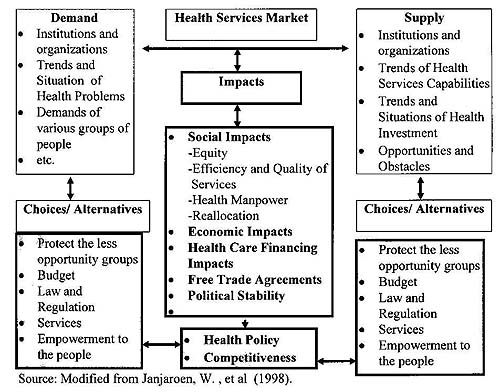
6. Social Impact and Responses
7. Economic Crisis:
Necessity and Opportunity to reassess priorities of Health Services Resources
- The most carefully laid plans are suddenly undermined by unpredicted national economic loss
- We have suddenly to make new priorities
- Health sector versus other sectors
- Within health sector
- Salaries
- Health services facilities
- Capital investment
- Disease control / preventive activities
- Health education / media
- Short term versus long term
- Local, national, regional
- New initiatives, i.e., Health Care Financing, Health Care Investment, etc.
- Equity, i.e., the rich and the poor, between sectors, between regions.
- Financial crisis
- Private hospitals, some are running out of money, bankruptcy.
- Drainage of manpower from public to private:
Private health sector interrupted results in the potential improvement of manpower situation in public sector conditional upon the availability of money to pay them.
- Shift of clientele from private to public health sector services, due to fall in income or unemployment of people.
- Consequent overloading of public health sector services.
- Can balance between public and private health sector be legislated based on experience of instability of private sector business methods exposed by crisis.
- Debt management, i.e., local and foreign investment
- Investment regulations
- Manpower policy adjustment
- Equity consideration
- Can disease controls / preventive activities are
a) streamlined, then
b) protected against cuts in crisis so to safeguard against costly increases in disease out breaks (communicable diseases) which would result in increasing debt burden.
- Time to readdress matter of comprehensive national health insurance encompassing all sectors. This might spread costs equitably.
8. Health Economics: Thai Experience
This list summarizes on going and completed health economics research throughout Thailand.
1. National Health System Research, i.e.,
2. Health Financing Research
- Voluntary Health Insurance.
- Social Security Scheme.
- Civil Service Medical Benefit Scheme (CSMBS).
3. Quality Improvement Research, i.e.,
4. Health Manpower Development Research, i.e.,
5. Health Behaviour Research, i.e.,
6. Health Situation and Trend Research, i.e.,
9. Summary of Health Economics Research Targets
Issues |
Equity |
Efficiency |
Quality |
| Health Insurance |
|
|
|
| Technology Assessment |
|
|
|
| Health Manpower |
|
|
|
| Role of
Private and Public |
|
|
|
Source: Modified from Janjaroen, W., et al, 1998.
Reference
CHE ‘96-’97 Annual Report. Centre for Health Economics, Faculty of Economics, Chulalongkorn University. 1998.
Health in Thailand 1995-1996. Bureau of Health Policy and Plan. Ministry of Public Health. Thailand. 1998.
Health System Research Institute Report of 1993-1996 (in Thai). Health System Research Institute. Bangkok, Thailand. 1997.
Supakankunti, S. Future Prospects of Voluntary Health Insurance in Thailand.
Takemi Paper No. 130, Harvard School of Public Health. 1997.
Thai Clinical Epidemiology Resource and Training Consortium Annual Report. Bangkok, Thailand. 1997.
Wattana S. Janjaroen, Siripen Supakankunti and others. “Strategy for Research in Health Economics: Present and Future” in Enabling Mechanisms for Health. Medical Research Division, The National Research Council of Thailand (NRCT), The Ministry of ScienceTechnology and Environment. 1998.
Wibulpolprasert, W., Tangcharoensathien, V. and Lertiendumrong, J. The Economic Crisis and Responses by Health Sectot in Thailand in 1997-1998. Paper presented to the Regional Consultation on Health Implications of Economic Crisis in the South-East Asia Region. Bangkok, Thailand. 23-25 March 1998.
![]()
![]()
![]()
![]()
![]()
![]()
Go back to the Main Page