This graphic is an ImageMap. You can either scroll down and read all the info or click on the waveform you'd like to read about and jump there.
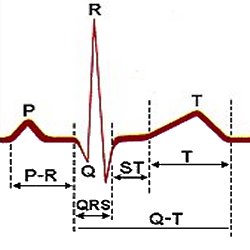
The normal EKG (ECG) is composed of a P wave, a QRS complex and a T wave. The P wave represents atrial depolarization and the QRS represents ventricular depolarization. The T wave reflects the phase of rapid repolarization of the ventricles.P Wave
The P wave is the first wave of the electrocardiogram and represents the spread of electrical impulse through the atrial musculature (activation or depolarization).The norms for this are:
Duration of not more than 0.11 seconds Amplitude of not more than 3mm in height and gently rounded, not pointed or notched. The normal deflection of the P wave is upright (positive) in leads I, II, and aVf. The deflection in AVl, and V3 to V6 are normally negative or biphasic, but may be positive. In leads III, V1 and V2 the deflection may be upright, biphasic, flat or inverted (negative) dependant upon the position of the heart in the body and the orientation of the leads. The P wave is normally inverted in lead aVr. There are several abnormalities that should be noted.
They are:
P-R Interval
The PR interval is measured from the beginning of the P wave to the beginning of the QRS complex. It reflects the time taken by the impulse to travel the entire distance from the SA Node to the ventricular muscle fibers. The normal duration for this is 0.12-0.20 seconds. Normally this interval varies with heart rate and is shorter at faster rates. Under certain circumstances, for instance if the conduction system is diseased or affected by Digitalis, the P-R interval may lengthen as the rate increases. Also if the atria are paced, the interval lengthens as the paced rate increases.
A prolonged interval, beyond normal limits (0.12-0.20 sec.), is considered evidence of AV block. An abnormally short P-R interval is cause for alarm as it is often seen in asociation with hypertension and paroxysms of tachycardia. The P-R interval is shortened when the impulse originates in the AV node rather than the SA node or when the passage of the impulse to the ventricle is accelerated as in Wolff-Parkinson-White syndrome (WPW).
QRS Complex
Probably the most important complex in the electrocardiogram is the QRS. It represents the spread of the electrical impulse through the ventricular muscle (depolarization).
The waves which make up this complex are labeled as follows:The first deflection , if it is negative (downward), is labeled the Q wave. The first positive (upright) delflection is labeled the R wave, whether it is predeceded by a Q wave or not. A negative deflection following an R wave is labeled an S wave. Any subsequent waveforms are labeled "primes". Positive being R', R'' etc.... Negative being S', S''. There are a number of features which should be routinely examined in the interpretation of the QRS complex.
The duration (QRS interval) which is measured from the beginning of the QRS complex to it's end. The normal duration of this interval is 0.05 to 0.10 seconds. A measurement of 0.12 seconds or more indicates abnormal intraventricular conduction and often indicates a block of one of the bundle branches or a ventricular arrhythmia. The amplitude ("voltage") has wide normal limits. An amplitude of 5 mm or less in all three standard leads is considered to be unhealthy. this is often seen coronary disease, cardiac failure, emphysema, and obesity to name a few.
The upper limit is variable from lead to lead, but generally is between 20 and 30 mm. Many factors can affect the amplitude besides the health of the heart, such as chest size, chest wall thickness, emphysema. These factors should always be taken into consideration before judging the voltage of any complex to be too high or too low.This section is barely started, lots more info to come.
S-T Segment
The S-T segment follows the QRS complex. The point at which it begins is called the J (junction) point. There are two aspects that should always be examined:
Its level relative to the baseline (elevated or depressed and how much). Its shape. Under normal circumstances the S-T segment is isoelectric or level with the T-P segment. It normally gently curves into the T wave.
T Wave
The T wave represents the period of recovery for the venticles (repolariztion). Generally we are concerned with three features: 1.) direction, 2.) shape, and 3.) height.The direction of the normal adult T wave is upright in leads I, II and V3-V6. It is inverted in aVr. And it is inverted in leads III, aVl, aVf, V1 and V2. The normal shape of the T wave is slightly rounded and slightly asymetrical. Sharply pointed or grossly notched T waves should cause suspicion, although either feature can occur as a normal variant of the precordial leads. Notching can be an indication of pericarditis, and sharply pointed symmetrical T waves should make one suspicious of myocardial infarction(MI). The height of the T wave also has diagnostic importance. Normal height in the limb leads is not above 5 mm and is not above 10 mm in any precordial lead. Unusually tall T waves indicate MI, but can be seen in ischemia without infarction. Tall T waves are also seen in patients with hyperkalemia, CVAs, and sometimes in psychotic patients.
Q-T Interval