| The Pityriasis
Rosea !!! The sixth illness ??? La Pitiriasis
Rosada !!! La
sexta enfermedad ???
EDITORIAL ESPANOL
================= Hola amigos de la red, DERMAGIC de
nuevo con ustedes con el tema: PITIRIASIS ROSADA ACTUALIZACION. La ptiriasis Rosada es
una de esas enfermedades ancestrales, descrita por primera vez por GIBERT, en
1860. Otros Autores la han descrito con otros nombres, entre ellos: Eritema
Anulatum (Rayer), Herpes tonsurans maculoso y escamoso (Hebra), Liquen annulatum
serpiginoso (Wilson), pitiriasis circinada (Honrad), Pitiriasis diseminada (Hardy),
Pitiriasis marginada y circinada ((Vidal), Pitiriasis Rubra aigu disseminee (Bazin),
Seudoexantema eritemato descamativo (Besnier), Roseola Annulata (Wilan), Roseola
furfuracea herpetiforme (Beherend) y Roseola escamosa (Nicolas y Chapard).
Hoy en dia han pasado mas de 140 años desde la epoca que inmortalizo a GIBERT, y
se discuten los probables agentes causales de la enfermedad, entre ellos
bacterias y virus de la familia herpes, siendo estos ultimos los virus HERPES 6
y 7 los mas asociados con la enfermedad.
Es de notar que hay estudios donde se demuestra la efectividad de la
ERITROMICINA en el tratamiento de la enfermedad, yo particularmente he obtenido
buenos resultados en muchos casos con el antibiotico CEFALOSPORINAS y en otros
casos el antiviral VALACICLOVIR tambien ha resultado exitoso.
La pitiriasis rosada tiene un comportamiento netamente ESTACIONAL, donde en una
epoca del año (otoño e invierno) ocurren la mayoria de los casos, es mas frecuente en la mujer, y
aunque CLASICAMENTE no produce lesiones en cara, palmas y plantas, yo he visto
tales manifestaciones y estan descritas en la literatura.
La clasica macula o PLACA HERALDICA representa el inicio de la enfermedad y luego se
presenta el brote metamerico en "arbol de navidad" clasico de tal enfermedad,
por lo general son placas ovales, pero se han descrito variantes, VESICULARES,
PAPULARES Y PURPURICAS de la misma afeccion.
Un dato interesante es que en la mayoria de los casos NO REPITE LA ENFERMEDAD,
aunque en algunos casos a los años puede presentarse una segunda manifestacion
IGUAL a la primera vez. Pero por lo general deja INMUNIDAD DEFINITIVA. Tambien
se han descrito erupciones PITIRIASIS ROSADA LIKE, inducida por medicamentos.
Si tomamos como valida la RECIENTE afirmacion que la PITIRIASIS ROSADA esta
asociada a los HERPES VIRUS 6 Y 7, y que estos pueden encontrarse en la saliva
de personas sanas, podriamos LANZAR la TEORIA de que EL CAMBIO ESTACIONAL
(otoño, invierno) ACTIVA la virulencia de estos virus, provocando la enfermedad,
al cambiar el clima de nuevo (verano), LOS VIRUS PIERDEN ACTIVIDAD y disminuye
el porcentaje de casos.
Porque NO TODOS MANIFIESTAN LA ENFERMEDAD, ?? como TODAS las clasicas eruptivas
??, se explicaria por el grado de proteccion inmunologica que tienen las PERSONAS
CONTRA ESTOS HERPES VIRUS. TAMBIEN EXISTEN PERSONAS A LAS CUALES NUNCA LES DIO
ALGUNA DE LAS CLASICAS ERUPTIVAS !!! con o sin inmunizacion !!!
La clasica PITIRIASIS ROSADA se comporta CASI igualmente en todos los pacientes,
con un RASH eruptivo luego de un tiempo de incubacion marcado por la placa
HERALDICA, se han descrito casos de lesiones en mucosas (boca), mas del 98% de
los casos deja inmunidad definitiva y ahora se le ha
comprobado su ETIOLOGIA INFECCIOSA ( principalmente VIRAL)
En base a estos HECHOS,
particularmente PROPONDRIA reclasificarla y colocarla en el GRUPO de las enfermedades ERUPTIVAS, la SEXTA enfermedad despues de el SARAMPION, RUBEOLA, VARICELA,
EXANTEMA SUBITO (Roseola infantil) y el ERITEMA INFECCIOSO (quinta enfermedad).
Recordemos que el ERITEMA INFECCIOSO ha sido asociado al VIRUS parvovirus
B19, y el EXANTEMA SUBITO al VIRUS HERPES 6. De manera me parece LOGICO colocar
a la pitiriasis ROSADA DENTRO de este grupo, me refiero a la clasica enfermedad,
NO A LA INDUCIDA por medicamentos u otros agentes, QUE REALMENTE son eccemas
similares (LIKE) a la Pitiriasis.Rosada.
En las referencias los hechos
Dr Jose Lapenta R.
ENGLISH EDITORIAL
=================
Hello friends of the net, DERMAGIC again with you with the topic: PITYRIASIS
ROSEA,
AN UPDATE. The Pityriasis Rosea is one of those ancestral illnesses, described
for the first
time by GIBERT, in 1860. Other Authors have described it with other names, among
them:
Erythema Annulatum (Rayer), Herpes tonsurans maculous et squamous (Strand),
Lichen
annulatus serpiginous (Wilson), pityriasis circine (Horand), Piyiriasis
dissemine (Hardy),
Pityriasis circinee et marginee ((Vidal), Pityriasis Rubra aigu disseminee
(Bazin), Pseudoexantheme erytematodescuamatif (Besnier), Roseola Annulata (Wilan),
Roseola furfuracea herpetiformis (Beherend) and Roseola squamosa (Nicolas and
Chapard).
Today in day they have lapsed but of 140 years from the time that I immortalize
GIBERT,
and the probable causal agents of the illness are discussed, among them
bacterias and virus,
of the family HERPES, being these last ones the virus HERPES 6 and 7 those but
associated
with the illness.
It is of noticing that there are studies where the effectiveness of the
erythromycin is
demonstrated in the treatment of the illness, I particularly have obtained good
results in many
cases with the antibiotic CEPHALOSPORIN, and in other cases the antiviral
VALACYCLOVIR
has also been successful.
The PITYRIASIS ROSEA has a behavior highly SEASONAL, where in a time of the year
they are presented most of the cases (autumn and winter) , it is but frequents
in the woman,
and although CLASSICALLY it doesn't produce lesions in face and palms and plants,
I
have seen such manifestations and they are described in the literature.
The classic HERALDIC MACULE or PATCH represents the beginning of the disease and
then the metameric sprout is presented in "Christmas tree" pattern classic of
such an illness, in
general they are oval plaques, but variants, VESICULAR, PAPULAR AND PURPURIC of
the same affection have been described.
An interesting fact is that in most of the cases it doesn't REPEAT THE ILLNESS,
although in
some cases a years a second manifestation SIMILAR to the first time can be
presented. But
in general she leaves DEFINITIVE IMMUNITY. Also eruptions PITYRIASIS ROSEA LIKE has been described, induced by medications.
If we take like real truth the RECENT statement that the PITYRIASIS ROSEA is
associated
to the HERPES VIRUS 6 AND 7, and that these they can be isolated from the saliva
of
healthy people, we could THROW the THEORY that THE SEASONAL CHANGE active
the virulence of these virus, causing the illness, when changing the climate
again (summer),
THE VIRUS LOSES ACTIVITY and it diminishes the percentage of cases.
WHY NOT ALL MANIFEST THE ILLNESS?? as ALL the classics eruptives ??, it would be
explained by the grade of immunologic protection that they have PEOPLE AGAINST
THESE HERPES VIRUS. PEOPLE ALSO EXIST TO WHICH NEVER SUFFERED THEM SOME OF THE
CLASSIC ERUPTIVES !!!, with or without immunization !!!
The classic PITYRIASIS ROSEA behaves equally particularly in all the patients,
with an eruptive RASH after a time of incubation marked for the
HERALD PATCH, cases of lesions have been described in mucous (mouth), but of 98%
of the cases leaves definitive immunity, and now it
has been checked its INFECTIOUS ETIOLOGY(mainly VIRAL)
Based on these FACTS, particularly I would INTEND to
reclassify it and to place it in the GROUP of the ERUPTIVE illnesses, the SIXTH
illness after the MEASLES, RUBELLA, CHICKEN POX, EXANTHEMA SUBITUM (infantile
Roseola) and the ERYTHEMA INFECTIOSUM (fifth illness).
Let us remember that the ERYTHEMA INFECTIOSUM has been associated to the VIRUS
parvovirus B19, and the EXANTHEM SUBITUM to the VIRUS HERPES 6. In way I find
LOGICAL to place to the PITYRIASIS ROSEA inside this group, I refer to the
classic
illness, NOT TO THE ONE INDUCED for medications or other agents, THAT they are
REALLY similar eczemas (LIKE) to the Pitiyriasis.Rosea.
In the references the facts
Dr José Lapenta R.
=======================================================
REFERENCIAS BIBLIOGRAFICAS/ BIBLIOGRAPHICAL REFERENCES
=======================================================
1.) Papular pityriasis rosea.
2.) Human herpes virus-like particles in pityriasis rosea lesions: an electron
microscopy study.
3.) Human herpesviruses 6 and 7.
4.) Human herpesvirus 7 in dermatology: what role does it play?
5.) [Myerson nevus as a primary patch of Gibert pityriasis rosea. A case report]
6.) Rash orientation in pityriasis rosea: a qualitative study.
7.) Skin diseases associated with human herpesvirus 6, 7, and 8 infection.
8.) Collarette scaling in pityriasis rosea demonstrated by digital
epiluminescence dermatoscopy.
9.) [Etiopathogenic importance of human herpes viruses type 6, 7 and 8 in
manifestations of certain skin diseases]
10.) Prospective case-control study of chlamydia, legionella and mycoplasma
infections in patients with pityriasis rosea.
11.) Pityriasis rosea is associated with systemic active infection with both
human herpesvirus-7 and human herpesvirus-6.
12.) Detection of human herpesvirus 7 in pityriasis rosea by nested PCR.
13.) An epidemiological study of pityriasis rosea in the Eastern Anatolia.
14.) Human herpesvirus 7 in patients with pityriasis rosea. Electron microscopy
investigations and polymerase chain reaction in mononuclear cells, plasma and
skin.
15.) A pityriasis rosea-like eruption secondary to bacillus Calmette-Guerin
therapy for bladder cancer.
16.) UVB phototherapy for pityriasis rosea: a bilateral comparison study.
17.) Pityriasis rosea Gibert: detection of Legionella micdadei antibodies in
patients.
18.) Pityriasis rosea-like eruption after bone marrow transplantation.
19.) Tongue and cheek: oral lesions in pityriasis rosea.
20.) Pityriasis rosea and discoid eczema: dose related reactions to treatment
with gold.
21.) [Pityriasis rosea-like skin eruptions caused by captopril]
22.) Recurrent pityriasis rosea. New episodes every year for five years. A case
report.
23.) Pityriasis rosea-like eruption associated with BCG vaccination.
24.) [Vesicular pityriasis rosea]
25.) [Benign familial chronic pemphigus and pityriasis rosea. Clinical aspects
and histology of the coexistence of both dermatoses]
26.) Human herpesvirus 6 and 7 DNA in peripheral blood leucocytes and plasma in
patients with pityriasis rosea by polymerase chain reaction: a prospective case
control study.
27.) The human herpesviruses and pityriasis rosea: curious covert companions?
28.) Pityriasis rosea is not associated with human herpesvirus 7.
29.) Association of pityriasis rosea with human herpesvirus-6 and human
herpesvirus-7 in Taipei.
30.) Epidemiological study of human herpesvirus-6 and human herpesvirus-7 in
pityriasis rosea.
31.) Lack of evidence of active human herpesvirus 7 (HHV-7) infection in three
cases of pityriasis rosea in children.
32.) Pityriasis rosea associated with herpesvirus 7 DNA.
33.)Pityriasis rosea: one virus, two viruses, more viruses?
34.) Reactivation of human herpesvirus 6 in pityriasis rosea.
35.) Absence of picornavirus genome in pityriasis rosea.
36.) Human herpesvirus 7 in pityriasis rosea.
37.) Detection of human herpesvirus 7 in patients with pityriasis rosea and
healthy individuals.
38.) The association of pityriasis rosea with cytomegalovirus, Epstein-Barr
virus and parvovirus B19 infections - A prospective case control study by
polymerase chain reaction and serology.
39.) Pityriasis rosea associated with imatinib (STI571, Gleevec).
40.) Erythromycin in pityriasis rosea: A double-blind, placebo-controlled
clinical trial.
41.) A Remarkable Result of a Double-Masked, Placebo-Controlled Trial of
Erythromycin in the Treatment of Pityriasis Rosea.
42.) Case Clustering in Pityriasis Rosea
A Multicenter Epidemiologic Study in Primary Care Settings in Hong Kong
43.) Pityriasis rosea--a virus-induced skin disease? An update.
======================================================
HERPES VIRUS 6, 7 AND 8 … MORE
======================================================
======================================================
44.) Association between human herpesvirus type 6 and type 7, and
cytomegalovirus disease in heart transplant recipients.
45.) Invasion by human herpesvirus 6 and human herpesvirus 7 of the central
nervous system in patients with neurological signs and symptoms.
46.) Association of human herpesvirus 6 and human herpesvirus 7 with
demyelinating diseases of the nervous system.
47.) [Detection of human herpesvirus type 6, human herpesvirus type 7,
cytomegalovirus and human papillomavirus in cutaneous AIDS-associated Kaposi's
sarcoma]
48.) Influenza encephalopathy associated with infection with human herpesvirus 6
and/or human herpesvirus 7.
49.) Human herpesvirus 6 and human herpesvirus 7 infections in renal transplant
recipients and healthy adults in Turkey.
50.) Detection of human herpesvirus-6 DNA in peripheral blood and saliva.
51.) Human herpesvirus-6 and human herpesvirus-7 in the bone marrow from healthy
subjects.
52.) Lymphomatoid papulosis and human herpesviruses--A PCR-based evaluation for
the presence of human herpesvirus 6, 7 and 8 related herpesviruses.
53.) Presence of human herpesvirus 6 variants A and B in saliva and peripheral
blood mononuclear cells of healthy adults.
54.) Detection of human herpesvirus 6 DNAs in samples from several body sites of
patients with exanthem subitum and their mothers by polymerase chain reaction
assay.
55.) Human herpesvirus-6 and human herpesvirus-7 infections in bone marrow
transplant recipients.
56.) High prevalence of HHV-6 DNA in peripheral blood mononuclear cells of
healthy individuals detected by nested-PCR.
57.) Clinical features and viral excretion in an infant with primary human
herpesvirus 7 infection.
=======================================================
=======================================================
1.) Papular pityriasis rosea.
=======================================================
Cutis 2002 Jul;70(1):51-5; quiz 48
Bernardin RM, Ritter SE, Murchland MR.
David Grant Medical Center, Travis Air Force Base, Fairfield, California, USA.
Pityriasis rosea (PR) is a seasonal papulosquamous disorder that can be easily
confused with a wide variety of similar appearing cutaneous disorders. This is
particularly evident in its atypical papular form. We present a case report of
atypical papular PR, along with a discussion of clinical presentation,
histologic criteria, proposed etiology, and treatment options. Papular PR is
atypical, presenting in a minority of patients, and may pose a diagnostic
challenge. Being familiar with these atypical characteristics will facilitate
accurate and timely diagnosis.
=======================================================
2.) Human herpes virus-like particles in pityriasis rosea lesions: an electron
microscopy study.
=======================================================
J Cutan Pathol 2002 Jul;29(6):359-61
Drago F, Malaguti F, Ranieri E, Losi E, Rebora A.
Section of Dermatology, Department of Health Sciences, DiSEM, University of
Genoa, Viale Benedetto XV 7, 16132 Genoa, Italy. [email protected]
BACKGROUND: In a previous study we detected virions with electron microscopy
features of human herpes viruses in the supernatant of cocultured mononuclear
cells from patients with acute pityriasis rosea. Because of their morphology and
of polymerase chain reaction studies, we ascribed them to human herpes virus 7.
OBJECTIVE: To find such virions in the lesional skin of pityriasis rosea
patients. METHODS: Skin specimens from lesions of 21 patients with acute
pityriasis rosea were examined by elecron microscopy. RESULTS: In 15 (71%)
patients, human herpes virus particles in various stages of morphogenesis were
detected. Mature enveloped virions appeared as typical human herpes virus
virions, measuring about 160-200 nm in diameter and containing an electrodense
cylindrical core, a capsid, an envelope with typical spikes and a very distinct
tegument layer between the capsid and the envelope. They were very similar to
those we reported in the supernatant of co-cultured circulating mononuclear
cells from patients with pityriasis rosea. CONCLUSION: Our results confirm our
previous findings and provides further evidence of a viral etiology for
pityriasis rosea.
=======================================================
3.) Human herpesviruses 6 and 7.
=======================================================
Dermatol Clin 2002 Apr;20(2):301-6
De Araujo T, Berman B, Weinstein A.
Department of Dermatology and Cutaneous Surgery, University of Miami School of
Medicine, Miami, FL 33136, USA.
Human herpesviruses 6 and 7 are newly discovered viruses that belong to the
genus Roseolavirus within the subfamily Betaherpesvirinae. These ubiquitous
viruses may cause primary or chronic persistent infection or remain in a state
of latency for many years, until a decrease in the immunologic state of the host
leads to reactivation of infection. Several diseases have been linked with HHV-6
and HHV-7. In the dermatologic arena, a definite association has been proven
only for HHV-6 and exanthema subitum (roseola infantum), whereas the role of HHV-7
in the pathogenesis of pityriasis rosea remains a matter of debate.
=======================================================
4.) Human herpesvirus 7 in dermatology: what role does it play?
=======================================================
Am J Clin Dermatol 2002;3(5):309-15
Kempf W.
Department of Dermatology, University Hospital, Zurich, Switzerland. [email protected]
Human herpesvirus 7 (HHV-7) was discovered in 1989 as a new member of the beta-herpesvirus
subfamily. Primary infection occurs early in life and manifests as exanthema
subitum, or other febrile illnesses mimicking measles and rubella. Thus, HHV-7
has to be considered as a causative agent in a variety of macular-papular rashes
in children. In addition, HHV-7 was found in some cases of other inflammatory
skin disorders, such as psoriasis. There are controversial data on the detection
of HHV-7 in pityriasis rosea, but so far there is not enough evidence for a
pathogenetic association of HHV-7 with this exanthematic skin disease. Although
HHV-7 can be found in some cases of Hodgkin's disease, there are no data
supporting a direct causative role in this lymphoma type nor in other nodal or
primary cutaneous lymphomas. In various epidemiologic forms of Kaposi's sarcoma,
infection of monocytic cells with HHV-7 was demonstrated, which may indirectly
influence tumor biology. In the context of immunosuppression, HHV-7 has recently
been identified as an emerging pathogen in transplant recipients and may
exacerbate graft rejection in renal transplant recipients. The ability of HHV-7
to induce cytokine production in infected cells could make HHV-7 an important
pathogenetic co-factor in inflammatory and neoplastic disorders. Moreover, the
restricted cellular tropism of HHV-7 may render this virus an interesting vector
for gene therapy. Thirteen years after the discovery of HHV-7, there has been
considerable progress in characterizing its genetic structure, virus-induced
effects on infected host cells and in the development of diagnostic tools.
Nevertheless, the role of HHV-7 in various skin diseases and the clinical
manifestations of reactivation of HHV-7 infection have still to be defined.
=======================================================
5.) [Myerson nevus as a primary patch of Gibert pityriasis rosea. A case report]
======================================================= Hautarzt 2002
May;53(5):338-41
[Article in German]
Hofer T.
Dermatologie FMH, Winkelriedstrasse 10, CH-5430 Wettingen. [email protected]
There are only few articles in literature which discuss the association between
Meyerson's naevi and Pityriasis rosea. And when so, the discussion is done in a
controversial way. Here an 18 year old man is presented who visits the
outpatient clinic. He has a ten day history of a solitary Meyerson's naevus on
his back. Over the next three weeks this naevus will develop to the typical
herold patch followed by the classical exantheme of Pityriasis rosea. CONCLUSION:
Halo dermatitis associated with Pityriasis rosea don't represent Meyerson's
naevi. But they reflect the rare "nevocentric" property of a not so rare
dermatose.
=======================================================
6.) Rash orientation in pityriasis rosea: a qualitative study.
=======================================================
Eur J Dermatol 2002 May-Jun;12(3):253-6
Chuh AA.
University of Hong Kong, Shop B5, Ning Yeung Terrace, 78 Bonham Road, Ground
Floor, Hong Kong. [email protected]
Rash orientation in pityriasis rosea (PR) has been described as Christmas-tree
pattern, inverted Christmas-tree pattern, fir tree pattern, parallel to the ribs
or along skin cleavage lines. We retrieved clinical photographs of 11 patients
diagnosed as having PR over a two-year period for qualitative study of rash
orientation. We found that Langer's cleavage lines are the most appropriate
description. All three components of these lines on the trunk, i.e. V-shaped
pattern on upper chest and upper back, circumferential pattern around the
shoulders and hips, and transverse pattern on the lower anterior trunk and lower
back, are demonstrated by most patients. We believe with the present state of
knowledge, the mechanism for PR following Langer's lines is best considered
unknown. We advocate abandoning other descriptions which might cause confusion
to students and trainee physicians.
=======================================================
7.) Skin diseases associated with human herpesvirus 6, 7, and 8 infection.
=======================================================
J Investig Dermatol Symp Proc 2001 Dec;6(3):197-202
Blauvelt A.
Dermatology Branch, National Cancer Institute, Bethesda, Maryland 20892-1908,
USA. [email protected]
Relatively recently, the discovery and analysis of three new human herpesviruses,
human herpesvirus (HHV)-6, HHV-7, and Kaposi's sarcoma-associated herpesvirus (KSHV),
also known as HHV-8, has contributed greatly to our understanding of the
pathogenesis of several common dermatoses. HHV-6 and HHV-7 are closely related
beta-herpesviruses that have been linked with roseola (mostly HHV-6), severe
drug eruptions (HHV-6), and pityriasis rosea (mostly HHV-7). KSHV is a gamma-herpesvirus
that is now believed to be the long sought after etiologic agent of Kaposi's
sarcoma. The evidence for these skin disease associations and key findings from
recent basic science investigations on viral pathogenesis are discussed in this
review. In addition, possible therapeutic implications of these research studies
are explored.
=======================================================
8.) Collarette scaling in pityriasis rosea demonstrated by digital
epiluminescence dermatoscopy.
=======================================================
Australas J Dermatol 2001 Nov;42(4):288-90
Chuh AA.
Department of Medicine, University of Hong Kong, Hong Kong, ROC. [email protected]
Collarette scaling is a characteristic sign in pityriasis rosea. The use of
digital epiluminescence dermatoscopy is proposed to assist in the recognition of
this sign as this technique can magnify the lesions, eliminate other epidermal
changes, and demonstrate the morphology and direction of scaling.
=======================================================
9.) [Etiopathogenic importance of human herpes viruses type 6, 7 and 8 in
manifestations of certain skin diseases]
=======================================================
Med Pregl 2001 Sep-Oct;54(9-10):459-63
[Article in Serbo-Croatian (Roman)]
Poljacki M, Rajic N, Matic M.
Klinika za kozno-venericne bolesti, 21000 Novi Sad, Hajduk Veljkova 1-3. [email protected]
INTRODUCTION: In the past few years new human herpes viruses (HHV): HHV-6, -7
and -8 have been discovered. According to the most recent literature, they might
have an important role in etiopathogenesis of some dermatological diseases.
HUMAN HERPESVIRUS 6: HHV-6 was isolated in 1984 from peripheral blood
lymphocytes of AIDS patients and patients with different lymphoproliferative
diseases. Up to now, two variants of this virus have been identified, A and B,
which differ in genetic, biological and immunological characteristics. The
etiological importance of variant A, has not yet been clarified, while variant B
is considered to be the major cause of many diseases, such as exanthema subitum
in infants. In many cases primary infection is associated with elevated
temperature, without rash. HUMAN HERPESVIRUS 7: HHV-7 was isolated in 1990 from
activated peripheral blood CD4+ T cells of healthy persons. The virus is
ubiquitous and more than 80% of babies and infants are affected. Presence of DNA
sequences of this virus in mononuclear cells of peripheral blood, skin and
plasma of pityriasis rosea patients, points to possible connection between this
illness and HHV-7 infection. HUMAN HERPESVIRUS 8: HHV-8 was first identified in
tissue samples of patients with Kaposi's sarcoma associated with AIDS in 1994.
DNA virus sequences were also isolated in HIV negative persons with Kaposis's
sarcoma. Presence of virus can be established in mononuclear cells of peripheral
blood, endothelial cells that cover vascular spaces and spindle cells within
skin changes. Modes of transmission are still not clarified. However, HHV-8 was
identified in some other dermatological diseases as well.
=======================================================
10.) Prospective case-control study of chlamydia, legionella and mycoplasma
infections in patients with pityriasis rosea.
=======================================================
Eur J Dermatol 2002 Mar-Apr;12(2):170-3
Chuh AA, Chan HH.
The Bonham Surgery, Shop B5, Ning Yeung Terrace, 78 Bonham Road, Ground Floor,
Hong Kong, China. [email protected]
A double-blind placebo-controlled trial reported the benefit of erythromycin in
treating pityriasis rosea (PR), a postulated mechanism being the eradication of
bacteria susceptible to erythromycin. The aim of this study was to investigate
the association between PR and Chlamydia pneumoniae, C. trachomatis, Legionella
longbeachae, L. micdadei, L. pneumophila, and Mycoplasma pneumoniae infections.
We recruited 13 patients aged seven to 46 years (mean: 26.8 years) diagnosed to
have PR in a primary care setting in 18 months. Lesional histopathology was
arranged for atypical cases. Clotted blood was collected at initial presentation
and four weeks later. Controls were 13 paired age-and-sex-matched patients
requiring blood collection for non-dermatological diseases. Serology tests were
performed in parallel but were read "blinded" on the acute and convalescent
specimens of patients and the control subjects. The serology profiles were not
diagnostic of active infection by any of the bacteria studied for all 13
patients. Two patients had four-fold increase in IgG titres against C.
pneumoniae, with IgM being negative. Two patients had IgM detectable against L.
pneumophila serotype 6 and M. pneumoniae respectively, with no significant rise
of the specific IgG. These patients had no symptom or sign of chest infection.
The seroprevalence and IgG titres of the study patients for the bacteria
investigated were insignificantly different from those of control subjects. We
conclude that the bacteria investigated in this study do not play a significant
role in the pathogenesis of PR. We believe that anti-inflammatory and
immunomodulatary effects might contribute towards the action of erythromycin, if
any, in PR.
=======================================================
11.) Pityriasis rosea is associated with systemic active infection with both
human herpesvirus-7 and human herpesvirus-6.
=======================================================
J Invest Dermatol 2002 Oct;119(4):793-7
Comment in:
J Invest Dermatol. 2002 Oct;119(4):779-80.
Watanabe T, Kawamura T, Jacob SE, Aquilino EA, Orenstein JM, Black JB, Blauvelt
A.
Dermatology Branch and Division of Cancer Treatment and Diagnosis, Center for
Cancer Research, National Cancer Institute, Howard Hughes Medical Institute, NIH
Medical Research Scholar Program, Bethesda, Maryland, USA.
Pityriasis rosea is a common skin disease that has been suspected to have a
viral etiology. We performed nested polymerase chain reaction to detect human
herpesvirus-7, human herpesvirus-6, and cytomegalovirus DNA in lesional skin,
nonlesional skin, peripheral blood mononuclear cells, serum, and saliva samples
isolated from 14 pityriasis rosea patients. Viral mRNA expression and virion
visualization within lesional skin were studied by in situ hybridization and
transmission electron microscopy, respectively. By nested polymerase chain
reaction, human herpesvirus-7 DNA was present in lesional skin (93%),
nonlesional skin (86%), saliva (100%), peripheral blood mononuclear cells (83%),
and serum (100%) samples, whereas human herpesvirus-6 DNA was detected in
lesional skin (86%), nonlesional skin (79%), saliva (80%), peripheral blood
mononuclear cells (83%), and serum (88%) samples. By contrast, cytomegalovirus
DNA was not detected in these tissues. Control samples from 12 healthy
volunteers and 10 psoriasis patients demonstrated rare positivity for either
human herpesvirus-7 or human herpesvirus-6 DNA in skin or serum. By in situ
hybridization, infiltrating mononuclear cells expressing human herpesvirus-7 and
human herpesvirus-6 mRNA were identified in perivascular and periappendageal
areas in 100% and 75% pityriasis rosea skin lesions, respectively, compared to
herpesviral mRNA positivity in only 13% normal skin and psoriasis skin controls.
Transmission electron microscopy failed to reveal herpesviral virions in
pityriasis rosea lesional skin. Nested polymerase chain reaction and in situ
hybridization enabled detection of human herpesvirus-7 and human herpesvirus-6
in skin and other tissues isolated from patients with pityriasis rosea. These
results suggest that pityriasis rosea is associated with systemic active
infection with both human herpesvirus-7 and human herpesvirus-6.
=======================================================
12.) Detection of human herpesvirus 7 in pityriasis rosea by nested PCR.
=======================================================
Int J Dermatol 2002 Sep;41(9):563-
Karabulut AA, Kocak M, Yilmaz N, Eksioglu M.
Department of Dermatology, Ankara Education and Research Hospital, Refik Saydam
Hifzisihha Institute, Ministry of Health, Turkey.
BACKGROUND: Clinical presentation, immunologic, light microscopic, and electron
microscopic studies suggest a viral etiology for pityriasis rosea (PR).
OBJECTIVE: To evaluate whether human herpesvirus 7 (HHV-7) is an etiologic
factor for PR. PATIENTS AND METHODS: Twenty-one PR patients (12 female, nine
male) aged between 12 and 52 years, whose diagnoses were confirmed clinically
and histopathologically, were included in the study. The duration of the disease
was questioned. Tissue samples of 5-mm punch biopsy material were collected from
the patients and from six healthy volunteers (three female, three male) as the
controls. Nested polymerase chain reaction (PCR) with specific primers for HHV-7
DNA sequences (OPERON technologies Inc., HV-7S/HV-8A external sences and HV-10S/HV11A
internal sences) was performed on each tissue sample. Polymerase chain reaction
products were analyzed by electrophoresis on 2% agarose gels. After molecular
weight markers (Haphi174) had been placed and visualized on an ultraviolet
transilluminator, the gels were immersed and photographs were taken. RESULTS:
The mean age was 29.86 +/- 11.77 for the PR patients and 25.33 +/- 11.69 for the
controls. The mean duration of the disease was 16.28 +/- 15.74 days. Human
herpesvirus 7 DNA sequences were detected in six of the PR patients (28.57%).
The mean duration of the disease was calculated as 11.67 +/- 9.85 for the HHV-7-positive
patients (patient nos. 3, 4, 5, 7, 8, 9) and 18.13 +/- 17.05 for the HHV-7-negative
patients, and there was no statistically significant differences in either of
the groups (U = 29.5, W = 50.5, P = 0.2241, using the Mann-Whitney U and
Wilcoxon's rank sum W-tests). Nested PCR was negative for HHV-7 in all of the
specimens from the controls. There was no statistically significant difference
for the presence of HHV-7 DNA sequence between the PR patients and the controls
(P = 0.2843, Fisher's exact two-tail analysis test). CONCLUSION: Our results
failed to support a possible role for HHV-7 in the pathogenesis of PR.
=======================================================
13.) An epidemiological study of pityriasis rosea in the Eastern Anatolia.
=======================================================
Eur J Epidemiol 1998 Jul;14(5):495-7
Harman M, Aytekin S, Akdeniz S, Inaloz HS.
Department of Dermatology & Venerology, Faculty of Medicine, University of Dicle,
Diyarbakir, Turkey.
The purpose of this study was to investigate the epidemiological features of
pityriasis rosea (PR) in the Eastern Anatolia, Turkey. Three hundred ninety-one
patients (214 females, 177 males) with PR seen during the years 1992-1995 were
analyzed for annual incidence among dermatologic outpatients, sex, age, and
distribution by month and year. The average annual incidence was 0.75 per 100
dermatologic patients. PR was reported to be slightly more common in women by
margin of 1.2:1.0. Eighty-seven percent of the cases were between the ages of 10
and 39 years, with a peak in the 20-29 age group. The incidence of the disease
was much higher in the rainy and snowy months. No declining incidence was
observed over the years. Changes in incidence from year to year, though not
great, were statistically significant.
=======================================================
14.) Human herpesvirus 7 in patients with pityriasis rosea. Electron microscopy
investigations and polymerase chain reaction in mononuclear cells, plasma and
skin.
=======================================================
Dermatology 1997;195(4):374-8
Comment in:
Dermatology. 1998;196(2):275.
Dermatology. 1999;199(2):197-8.
Drago F, Ranieri E, Malaguti F, Battifoglio ML, Losi E, Rebora A.
Institute of Dermatology, University of Genoa, Italy.
BACKGROUND: Clinical evidence suggests a viral etiology for pityriasis rosea
(PR). OBJECTIVE: To evaluate human herpesvirus (HHV)-6 and HHV-7 as candidates
for the etiology of PR. METHODS: Blood and skin tissue from 12 patients with
acute PR, and 12 patients with other dermatoses were studied, as well as blood
samples from 25 healthy persons. Serum interferon (IFN)-alpha and IFN-gamma were
analyzed by ELISA. Analysis of morphological changes in cocultured peripheral
blood mononuclear cells (PBMC) and electron microscopy (EM) to identify viral
particles were performed. Polymerase chain reaction (PCR) with specific primers
for HHV-6 and HHV-7 DNA sequences was performed on the plasma and PBMC of
patients and healthy controls and on the skin of patients with PR and other skin
diseases. RESULTS: PR plasma contained detectable IFN-alpha and IFN-gamma,
whereas plasma from controls did not. PBMC from PR patients showed ballooning
cells and syncytia after 7 days in culture whereas PBMC from controls and
recovered PR patients did not. This cytopathic effect was also documented in a
PR patient who relapsed and in Sup-T1 cell cultures inoculated with the cell-free
supernatant from centrifuged cultured PBMC; in this supernatant, herpesvirus,
virions were detected by EM, PCR identified HHV-7 DNA in PBMC, plasma and skin
from all patients with active PR and in the PBMC only of 5 patients tested 10-14
months later. Weaker signals of HHV-7 DNA were detected in PBMC of 11 controls,
but not in their plasma. Skin was negative for HHV-7 in all control specimens.
CONCLUSIONS: Although the detection of HHV-7 DNA in PBMC and tissues does not
prove directly a causal role, HHV-7 DNA in cell-free plasma corresponds to
active replication which supports a causal relationship. We propose that PR is a
clinical presentation of HHV-7 reactivation.
=======================================================
15.) A pityriasis rosea-like eruption secondary to bacillus Calmette-Guerin
therapy for bladder cancer.
=======================================================
Cutis 1996 Jun;57(6):447-50
Honl BA, Keeling JH, Lewis CW, Thompson IM.
Dermatology Service, Brooke Army Medical Center, Fort Sam Houston, Texas, USA.
The use of bacillus Calmette-Guerin (BCG) for the treatment of bladder cancer
has been followed by reports documenting adverse reactions. Eruptions of the
skin have been included (although not well described) in the list of side
effects. We report a pityriasis rosea-like rash secondary to BCG therapy for
bladder cancer. Although the treatment was interrupted because of this reaction,
the medication was restarted later with only a mild transient recurrence of the
eruption.
=======================================================
16.) UVB phototherapy for pityriasis rosea: a bilateral comparison study.
=======================================================
J Am Acad Dermatol 1995 Dec;33(6):996-9
Leenutaphong V, Jiamton S.
Department of Dermatology, Siriraj Hospital, Mahidol University, Bangkok,
Thailand.
BACKGROUND: Pityriasis rosea is a common self-limiting disease. UV light has
been mentioned as helpful, but only a few studies substantiate this possibility.
OBJECTIVE: Our purpose was to evaluate the clinical efficacy of UVB phototherapy
in pityriasis rosea and the course of the disease after treatment. METHODS:
Seventeen patients with extensive pityriasis rosea were treated with unilateral
UVB phototherapy in a bilateral comparison study. One joule of UVA was used as a
"placebo" on the untreated side. The treatments were given five times per week
for 2 weeks. The rate of clearing was monitored by estimation of the severity
score. RESULTS: Ten daily erythemogenic exposures of UVB resulted in
substantially decreased severity of disease, greater than that on the untreated
side in 15 of 17 patients. The overall reduction of severity score showed a
significant difference after the third treatment; the UVB irradiation was
superior. However, during the follow-up period the two sides were
indistinguishable in regard to severity score (p = 0.6784). No significant
difference in pruritus was noted between the two sides (p > 0.1638). The
duration of disease did not relate to the success of UVB phototherapy.
CONCLUSION: During the treatment period UVB phototherapy resulted in decreased
severity of disease. However, the itching and the course of the disease were
unchanged.
=======================================================
17.) Pityriasis rosea Gibert: detection of Legionella micdadei antibodies in
patients.
=======================================================
Eur J Epidemiol 1995 Aug;11(4):459-62
Gjenero-Margan I, Vidovic R, Drazenovic V.
Epidemiology Service, Croatian National Institute of Public Health, Zagreb,
Croatia.
Some epidemiological and clinical characteristics of Pityriasis rosea Gibert has
led us to hypothesize that this disease may be the clinical manifestation of an
infection caused by legionellas. We have thus tested the sera of 36 patients ill
with Pityriasis rosea and 19 controls for Legionella pneumophila serogroup 1-6
and Legionella micdadei antibodies. These, who had the same age and sex
distribution as study patients, were receiving treatment for other diseases in
the same ward. Also tested were 200 sera from the voluntary blood donors from
the same region as study patients. Legionella micdadei antibodies were detected
in 12 (33.3%) Pityriasis rosea cases and in one (5.2%) control. They were
significantly more common in Pityriasis rosea cases than in either controls or
voluntary blood donor population. The findings to date encourage continued
research into the causative relationship between the Legionella micddadei
infection and the onset of Pityriasis rosea Gibert.
=======================================================
18.) Pityriasis rosea-like eruption after bone marrow transplantation.
=======================================================
J Am Acad Dermatol 1994 Aug;31(2 Pt 2):348-51
Spelman LJ, Robertson IM, Strutton GM, Weedon D.
Department of Dermatology, Royal Brisbane Hospital, Australia.
Bone marrow transplantation is associated with numerous cutaneous complications
that may be related to the underlying (preexisting) disease, to pretransplant
conditioning, to immunosuppression, to concomitant medication, or to graft-versus-host
reaction. We describe four bone marrow transplant recipients with the clinical
and histologic features of pityriasis rosea, a hitherto unreported association.
=======================================================
19.) Tongue and cheek: oral lesions in pityriasis rosea.
=======================================================
Cutis 1992 Oct;50(4):276-80
Vidimos AT, Camisa C.
Cleveland Clinic Foundation, Department of Dermatology A61, Ohio 44195-5032.
Fifty-one consecutive patients with clinical findings and history consistent
with pityriasis rosea underwent a complete oral examination to search for any
concomitant oral lesions. One case was omitted from the statistical analysis
because the results of a rapid plasma reagin test were positive. Of the fifty
remaining cases, eight patients (16 percent) were noted to have various oral
lesions, all of which were asymptomatic. These findings suggest that the actual
incidence of oral lesions in pityriasis rosea may be higher than previously
reported. A complete oral examination in a patient presenting with a
papulosquamous eruption may be helpful in ascertaining the diagnosis of
pityriasis rosea.
=======================================================
20.) Pityriasis rosea and discoid eczema: dose related reactions to treatment
with gold.
=======================================================
Ann Rheum Dis 1992 Jul;51(7):881-4
Wilkinson SM, Smith AG, Davis MJ, Mattey D, Dawes PT.
Department of Dermatology, North Staffordshire Health District, Stoke-on-Trent,
United Kingdom.
Sixteen cases of either a pityriasiform or discoid eczematous rash occurring in
patients with rheumatoid arthritis receiving treatment with gold (sodium
aurothiomalate and auranofin) were studied. The results suggest that this is a
dose related, not allergic, reaction to gold. The development of this rash is
not an absolute indication to stop treatment with gold. Control can often be
effected with potent topical steroids or a reduction in the dose or frequency of
treatment with gold.
=======================================================
21.) [Pityriasis rosea-like skin eruptions caused by captopril]
=======================================================
G Ital Dermatol Venereol 1990 Oct;125(10):457-9
[Article in Italian]
Ghersetich I, Rindi L, Teofoli P, Tsampau D, Palleschi GM, Lotti T.
Istituto di Clinica Dermosifilopatica, Universita degli Studi di Firenze.
Captopril is an antihypertensive drug that works by inhibiting the angiotensin-converting
enzyme and provokes increased levels of plasma quinine. In the case here
reported a picture of pityriasis rosea-like reaction is described. The frequency
of the observed and reported reactions by captopril suggests a particular
caution in the use of this drug.
=======================================================
22.) Recurrent pityriasis rosea. New episodes every year for five years. A case
report.
=======================================================
Acta Derm Venereol 1990;70(2):179-80
Halkier-Sorensen L.
Department of Dermatology and Venereology, Marselisborg Hospital, University of
Aarhus, Denmark.
A case of recurrent pityriasis rosea in a 39-year-old woman is presented. She
had her first attack of pityriasis rosea 5 years ago and new outbreaks followed
every year, in the spring. Her husband had a severe attack of pityriasis rosea 6
years ago. All laboratory investigations were normal and no explanation for the
many recurrences was found.
=======================================================
23.) Pityriasis rosea-like eruption associated with BCG vaccination.
=======================================================
Isr J Med Sci 1989 Oct;25(10):570-2
Kaplan B, Grunwald MH, Halevy S.
Department of Dermatology, Soroka Medical Center, Beer Sheva, Israel.
We report a case of a pityriasis rosea-like eruption in a 12-year-old boy
several days following BCG vaccination. It is suggested that the BCG vaccination
be included in the etiology of pityriasis rosea-like eruptions.
=======================================================
24.) [Vesicular pityriasis rosea]
=======================================================
Hautarzt 1988 Aug;39(8):524-6
[Article in German]
Strauss T, Kuhn A, Steigleder GK.
Universitats-Hautklinik Koln.
Pityriasis rosea is a frequently occurring skin disease of unknown aetiology.
Ten clinical forms of this disease are known, with predominance of the macular
type. We observed a healthy 24-year-old patient with the very rare vesicular
variant of pityriasis rosea, which has to be differentiated from vesicular virus
and drug-induced eruptions.
=======================================================
25.) [Benign familial chronic pemphigus and pityriasis rosea. Clinical aspects
and histology of the coexistence of both dermatoses]
=======================================================
Hautarzt 1988 May;39(5):324-7
[Article in German]
Winzer M.
Klinik fur Dermatologie und Venerologie, Medizinischen Universitat zu Lubeck.
We report the course of benign familial pemphigus (Hailey-Hailey disease) in a
45-year-old woman. While this condition was in remission the patient started to
suffer from pityriasis rosea. A biopsy of this coexisting dermatosis revealed
the typical features of Hailey-Hailey disease (suprabasal acantholysis) and of
pityriasis rosea within the same lesion.
=======================================================
26.) Human herpesvirus 6 and 7 DNA in peripheral blood leucocytes and plasma in
patients with pityriasis rosea by polymerase chain reaction: a prospective case
control study.
=======================================================
Acta Derm Venereol 2001 Aug-Sep;81(4):289-90
Chuh AA, Chiu SS, Peiris JS.
Department of Medicine, University of Hong Kong, China. [email protected]
An association between pityriasis rosea and human herpesvirus 7 (HHV-7) has been
reported but remains controversial. The purpose of the present study was to
investigate the association between HHV-6 and HHV-7 with pityriasis rosea.
Fifteen patients aged 6-54 years with a diagnosis of pityriasis rosea and 15 age-matched
controls were recruited. None of the patients had HHV-6 or HHV-7 DNA detected by
polymerase chain reaction in the acute or convalescent plasma specimen. In the
acute peripheral blood leucocytes specimen, 3 patients and one control had RHV-6
DNA detected (p=0.299; NS), while 7 patients and 5 controls had HHV-7 DNA
(p=0.355; NS). Antibody to HHV-6 was detected in the acute specimen of 13
patients and 13 controls, while antibody to HHV-7 was found in all 15 of
patients and controls. We thus found no evidence of recent HHV-6 or HHV-7
infection in patients with a diagnosis of pityriasis rosea.
=======================================================
27.) The human herpesviruses and pityriasis rosea: curious covert companions?
=======================================================
J Invest Dermatol 2002 Oct;119(4):779-80
Comment on:
J Invest Dermatol. 2002 Oct;119(4):793-7.
Breese Hall C.
University of Rochester School of Medicine and Dentistry, Rochester, New York,
U.S.A.
Publication Types:
Comment
======================================================
=======================================================
28.) Pityriasis rosea is not associated with human herpesvirus 7.
=======================================================
Kempf W, Adams V, Kleinhans M, Burg G, Panizzon RG, Campadelli-Fiume G, Nestle
FO.
Department of Dermatology, University Hospital, Zurich, Switzerland.
OBJECTIVE: To examine the proposed association between pityriasis rosea and
human herpesvirus 7 (HHV-7). DESIGN: A retrospective cross-sectional survey.
SETTING: University medical center in Switzerland. PATIENTS: Thirteen patients
with pityriasis rosea and 14 persons with normal skin (control subjects). MAIN
OUTCOME MEASURES: Detection of HHV-7-specific DNA sequences and antigen (85-kd
phosphoprotein [pp85]) by nested polymerase chain reaction and
immunohistochemical analysis, respectively. RESULTS: Human herpesvirus 7 DNA
sequences and expression of the HHV-7-specific immunodominant pp85 antigen were
found in 1 (8%) of 13 lesional skin biopsy specimens of pityriasis rosea. The
prevalence of HHV-7 DNA sequences and antigens is even slightly lower in
lesional skin of patients with pityriasis rosea than in clinically and
morphologically normal skin of 14 control persons, in 2 of whom (14%) HHV-7 DNA
sequences and antigens could be detected. CONCLUSION: The low detection rate of
HHV-7 DNA sequences and antigens argues strongly against a causative role for
HHV-7 in the pathogenesis of pityriasis rosea.
=======================================================
29.) Association of pityriasis rosea with human herpesvirus-6 and human
herpesvirus-7 in Taipei.
=======================================================
J Formos Med Assoc 2001 Jul;100(7):478-83
Wong WR, Tsai CY, Shih SR, Chan HL.
Department of Dermatology, Chang Gung Memorial Hospital, 199 Tung Hwa North Road,
Taipei, Taiwan.
BACKGROUND AND PURPOSE: Pityriasis rosea (PR) is a common papulosquamous skin
disease with unknown etiology. The possible relationship of PR with human
herpesvirus infection (HHV) has been extensively studied. This study used the
polymerase chain reaction (PCR) to investigate the presence of human herpesvirus
6 and 7 (HHV-6 and HHV-7) in 41 PR patients from two hospitals in Northern
Taiwan. The epidemiologic features of PR in patients were also studied. METHODS:
A total of 41 PR patients (11 males, 30 females) were enrolled in this study
from April 1999 to March 2000. PCR of skin biopsy specimens from 24 PR patients
was used to identify the existence of HHV-6 and HHV-7. Viral culture from PR
biopsy specimens was also performed. Blood from these patients was sampled for
Venereal Disease Research Laboratory tests. Skin biopsies from 20 age- and sex-matched
controls with other skin diseases were also subjected to PCR study. RESULTS: The
ages of the 41 PR patients ranged from 8 to 62 years. An increased incidence
(17/41) of PR episodes was observed during the spring. Both HHV-6 and HHV-7 DNA
was below the limit of detection in all biopsy specimens from patients and
healthy controls. Viral culture for HHV was negative in all patients. CONCLUSION:
The epidemiologic features of PR in this series are comparable to other studies
except for an exaggerated female predominance (male:female ratio 1:2.7). Our
data indicate a lack of association between HHV-6 and HHV-7 infection and PR.
=======================================================
30.) Epidemiological study of human herpesvirus-6 and human herpesvirus-7 in
pityriasis rosea.
=======================================================
Br J Dermatol 2000 Oct;143(4):795-8
Comment in:
Br J Dermatol. 2001 May;144(5):1090.
Kosuge H, Tanaka-Taya K, Miyoshi H, Amo K, Harada R, Ebihara T, Kawahara Y,
Yamanishi K, Nishikawa T.
Department of Dermatology, Tokyo Electric Power Hospital, 9-2 Shinanomachi,
Shinjuku-ku, Tokyo 160-0016, Japan. [email protected]
BACKGROUND: Pityriasis rosea (PR) is a common papulosquamous skin disorder that
is suspected to have an infectious aetiology. OBJECTIVES: We aimed to study the
role of human herpesvirus (HHV)-7 and HHV-6 in the pathogenesis of PR. METHODS:
We performed seroepidemiological studies (indirect immunofluorescence test) and
polymerase chain reaction (PCR) analysis for HHV-6 and HHV-7 in patients with
PR. Seventy-two serum samples and 37 samples of peripheral blood mononuclear
cells (PBMC) from 44 patients with PR were obtained. Twenty-five patients with
other skin disorders such as drug eruption, urticaria or herpes zoster were
studied as controls in the PCR analysis. RESULTS: HHV-7 DNA was detected in 13
of 30 (43%) samples of PBMC of the patients with PR and 14 of 25 (56%) samples
of PBMC of controls. HHV-6 DNA was detected in six of 29 (21%) patients with PR
and nine of 23 (39%) controls. Thus there was no difference in the prevalence of
HHV-6 or HHV-7 in PBMC between patients with PR and those with other skin
disorders. In the seroepidemiological study, two cases of at least a fourfold
rise in titre and five cases of a fourfold decrease in titre to HHV-7 antibody,
and two cases of a fourfold rise in titre and two cases of a fourfold decrease
in titre to HHV-6 antibody, were observed in 24 patients with PR. This
seroepidemiological study revealed antibody responses consistent with active
infection in several PR patients, but the greater proportion of the patients had
no definite increase in the antibody titres. CONCLUSIONS: We conclude that HHV-7
and HHV-6 may play a part in some patients with PR, but that other causative
agents may exist. Further analyses are needed to determine the causative agents
of PR.
=======================================================
31.) Lack of evidence of active human herpesvirus 7 (HHV-7) infection in three
cases of pityriasis rosea in children.
=======================================================
Pediatr Dermatol 2001 Sep-Oct;18(5):381-3
Chuh AA, Peiris JS.
Department of Medicine, University of Hong Kong, Hong Kong. [email protected]
Three cases of pityriasis rosea in Chinese children are presented. Using
polymerase chain reaction for detection of human herpesvirus 7 (HHV-7) DNA in
plasma and peripheral blood lymphocytes, we find no evidence of active HHV-7
infection.
=======================================================
32.) Pityriasis rosea associated with herpesvirus 7 DNA.
=======================================================
J Eur Acad Dermatol Venereol 2000 Jul;14(4):313-4
Offidani A, Pritelli E, Simonetti O, Cellini A, Giornetta L, Bossi G.
Publication Types:
Letter
=======================================================
=======================================================
33.)Pityriasis rosea: one virus, two viruses, more viruses?
=======================================================
Br J Dermatol 2001 May;144(5):1090
Comment on:
Br J Dermatol. 1999 Jan;140(1):169-70.
Br J Dermatol. 2000 Oct;143(4):795-8.
Drago F, Rebora A.
Publication Types:
Comment
Letter
=======================================================
=======================================================
34.) Reactivation of human herpesvirus 6 in pityriasis rosea.
=======================================================
J Dermatol 1999 Jan;140(1):169-70
Comment in:
Br J Dermatol. 2001 May;144(5):1090.
Yasukawa M, Sada E, MacHino H, Fujita S.
Publication Types:
Letter
=======================================================
=======================================================
35.) Absence of picornavirus genome in pityriasis rosea.
=======================================================
Arch Dermatol Res 1996 Dec;289(1):60-1
Aractingi S, Morinet F, Mokni M, Tieng V, Flageul B, Fermand JP, Dubertret L.
Unite de Dermatologie, Hopital Tenon, Paris, France.
=======================================================
=======================================================
36.) Human herpesvirus 7 in pityriasis rosea.
=======================================================
Lancet 1997 May 10;349(9062):1367-8
Drago F, Ranieri E, Malaguti F, Losi E, Rebora A.
Publication Types:
Letter
=======================================================
=======================================================
37.) Detection of human herpesvirus 7 in patients with pityriasis rosea and
healthy individuals.
=======================================================
Dermatology 1999;199(2):197-8
Comment on:
Dermatology. 1997;195(4):374-8.
Yoshida M.
Publication Types:
Comment
Letter
=======================================================
=======================================================
38.) The association of pityriasis rosea with cytomegalovirus, Epstein-Barr
virus and parvovirus B19 infections - A prospective case control study by
polymerase chain reaction and serology.
=======================================================
Eur J Dermatol 2003 Jan-Feb;13(1):25-8
Chuh AA.
Department of Medicine, The University of Hong Kong and Queen Mary Hospital,
Pokfulam, Hong Kong SAR, China.
A viral aetiology is suspected for pityriasis rosea (PR). The objective was to
investigate the association of PR with cytomegalovirus (CMV), Epstein Barr virus
(EBV) and parvovirus B19 infections. Patients with PR were recruited in a
primary care setting over 18 months. Blood was collected at initial presentation
and four weeks later. Controls were the next age-and-sex-matched patients
requiring blood collection for non-dermatological disease. Polymerase chain
reaction was performed for EBV and parvovirus B19 DNA. Serology was done for CMV,
EBV and parvovirus B19. 12 patients with PR and 12 control subjects were
recruited. No patient had viral DNA or significant antibody rise against any of
the viruses investigated. The seroprevalence of all three viruses and Ab titres
in the patients with PR were insignificantly different from those of control
subjects. Two patients had IgM detectable against CMV and EBV respectively.
Based on other investigation results, we believe that both IgM results were
caused by cross reactivity. PR is not associated with CMV, EBV or parvovirus B19
infections.
=======================================================
39.) Pityriasis rosea associated with imatinib (STI571, Gleevec).
=======================================================
Dermatology 2002;205(2):172-3
Konstantopoulos K, Papadogianni A, Dimopoulou M, Kourelis C, Meletis J.
First Department of Medicine, University of Athens School of Medicine at Laikon
Hospital, Athens, Greece. [email protected]
A tyrosine kinase inhibitor (STI571, Gleevec) has recently been applied in the
treatment of chronic myeloid leukemia. We present the first reported case of
pityriasis rosea occurring as a reaction to Gleevec in a woman with blast crisis
of this disorder. It is suggested that although coincidental, this exanthem may
be due to this agent. Copyright 2002 S. Karger AG, Basel
=======================================================
40.) Erythromycin in pityriasis rosea: A double-blind, placebo-controlled
clinical trial.
=======================================================
J Am Acad Dermatol 2000 Feb;42(2 Pt 1):241-4
Sharma PK, Yadav TP, Gautam RK, Taneja N, Satyanarayana L.
Department of Dermatology, Dr Ram Manohar Lohia Hospital, New Delhi, India.
BACKGROUND: The study stemmed from an incidental observation of improvement in 2
patients with pityriasis rosea while receiving erythromycin. OBJECTIVE: The
purpose of the study was to evaluate the efficacy of erythromycin in patients
with pityriasis rosea. METHODS: A double-blind, placebo-controlled clinical
study was performed in an outpatient setting in a major hospital. Ninety
patients over a period of 2 years were alternatively assigned to treatment group
or placebo group. Patients in the treatment group received erythromycin in
divided doses for 14 days. The response was categorized as complete response,
partial response, or no response. All patients were followed up for 6 weeks.
RESULTS: Both groups were comparable with regard to age at presentation, sex,
and average duration of disease at the time of reporting to the clinic. Upper
respiratory tract infection before the appearance of skin lesions was reported
in 68.8% of all patients. Complete response was observed in 33 patients (73.33%)
in the treatment group and none in the placebo group (P <.0001). CONCLUSION:
Oral erythromycin was effective in treating patients with pityriasis rosea.
=======================================================
41.) A Remarkable Result of a Double-Masked, Placebo-Controlled Trial of
Erythromycin in the Treatment of Pityriasis Rosea.
=======================================================
Arch Dermatol 2000 Jun;136(6):775-776
Bigby M.
Editor.
PMID: 10871946 [PubMed - as supplied by publisher]
=======================================================
=======================================================
42.) Case Clustering in Pityriasis Rosea
A Multicenter Epidemiologic Study in Primary Care Settings in Hong Kong
=======================================================
Arch Dermatol. 2003;139:489-493.
Antonio A. T. Chuh, MRCP(UK), MRCP(Irel), MRCPCH, DipDerm; Albert Lee, MPH,
FRACGP, FHKCFP, FHKAM(Family Medicine); Nicolas Molinari, PhD
Objectives To investigate the epidemiology of pityriasis rosea in primary care
settings in Hong Kong and to analyze for temporal clustering.
Design Retrospective epidemiologic study.
Setting Six primary care teaching practices affiliated with a university.
Patients Forty-one patients with pityriasis rosea, 564 patients with atopic
dermatitis (negative control condition), and 35 patients with scabies (positive
control condition).
Methods We retrieved all records of patients with pityriasis rosea, atopic
dermatitis, or scabies diagnosed in 3 years. We analyzed temporal clustering by
a method based on a regression model.
Results The monthly incidence of pityriasis rosea is negatively but
insignificantly correlated with mean air temperature (s = -0.41, P = .19) and
mean total rainfall (s = -0.34, P = .27). Three statistically significant
clusters with 7, 6, and 7 cases were identified (P = .03), occurring in the
second coldest month in the year (February), the second hottest month (July),
and a temperate month (April), respectively. For atopic dermatitis (negative
control condition), the nonclustering regression model was selected by Akaike
information criteria. For scabies (positive control condition), 1 cluster of 20
cases was detected (P = .03).
Conclusions Significant temporal clustering independent of seasonal variation
occurred in our series of patients with pityriasis rosea. This may be indicative
of an infectious cause.
From the Department of Medicine, University of Hong Kong (Dr Chuh); Department
of Community and Family Medicine, Chinese University of Hong Kong (Dr Lee); and
Department of Biostatistics, Institut Universitaire de Recherche Clinique,
University of Montpellier I, Montpellier, France (Dr Molinari). The authors have
no relevant financial interest in this article.
=======================================================
43.) Pityriasis rosea--a virus-induced skin disease? An update.
=======================================================
Arch Virol 2000;145(8):1509-20
Kempf W, Burg G.
Department of Dermatology, University Hospital, Zurich, Switzerland.
Pityriasis rosea (PR) is an acute, inflammatory skin disease of unknown cause.
Clinical and experimental findings indicate an infectious etiology of PR.
Various infectious agents including viruses have been proposed as causative
agents and their presence in PR samples has been extensively investigated.
Recently, human herpesvirus 7 was linked to PR, but contradictory findings have
been reported by various investigators. Here, we describe the features of PR
that suggest an infectious cause and review the data from viral studies in PR
reported in the literature. In addition, we present a pathogenetic model of PR
which may be helpful in planning and evaluating studies for the search of a
putative PR-associated virus. Based on the current state of knowledge, none of
the known viruses could, so far, be conclusively associated with PR.
======================================================
HERPES VIRUS 6, 7 AND 8 … MORE
======================================================
======================================================
44.) Association between human herpesvirus type 6 and type 7, and
cytomegalovirus disease in heart transplant recipients.
======================================================
Transplant Proc 2002 Feb;34(1):75-6
de Ona M, Melon S, Rodriguez JL, Sanmartin JC, Bernardo MJ.
Unidades de Trasplante Cardiaco y de Virologia, Servicios de Cardiologia y
Microbiologia I, Hospital Central de Asturias, Spain.
======================================================
45.) Invasion by human herpesvirus 6 and human herpesvirus 7 of the central
nervous system in patients with neurological signs and symptoms.
======================================================
Arch Dis Child 2000 Aug;83(2):170-1
Yoshikawa T, Ihira M, Suzuki K, Suga S, Matsubara T, Furukawa S, Asano Y.
Department of Pediatrics, Fujita Health University School of Medicine, Aichi,
Japan. [email protected]
METHODS: A total of 43 children with neurological signs and symptoms were
enrolled in the study. All children were suspected of having meningitis, and
lumbar punctures were performed. Human herpesvirus 6 (HHV-6) and HHV-7 DNA was
detected in cerebrospinal fluid (CSF) and peripheral blood mononuclear cells (PBMC)
by nested polymerase chain reaction. RESULTS: Most patients had detectable serum
antibody to both HHV6 and 7. HHV6 DNA was detected in PBMC of 15 patients and in
CSF cell pellet of seven. Corresponding figures for HHV7 were 28 and 6.2/7, and
5/6 with CSF viral DNA also had it in PBMC, respectively. No viral DNA was
detected in CSF supernatants. The seven HHV6 CSF viruses were all variant B.
CONCLUSION: These data suggest that HHV-7 may invade the CNS.
======================================================
46.) Association of human herpesvirus 6 and human herpesvirus 7 with
demyelinating diseases of the nervous system.
======================================================
J Neurovirol 2001 Dec;7(6):564-9
Tomsone V, Logina I, Millers A, Chapenko S, Kozireva S, Murovska M.
August Kirchenshtein Institute of Microbiology and Virology, University of
Latvia, Ratsupites st. 1, Riga LV-1067, Latvia. [email protected]
Peripheral blood mononuclear cells and plasma of 113 patients with neurological
disorders and 150 blood donors were analyzed for HHV-6 and HHV-7 sequences by
PCR. The prevalence of HHV-6 was significantly higher in patients with multiple
sclerosis (P < 0.01) than in cases of nondemyelinating diseases of the central
and demyelinating diseases of the peripheral nervous systems and blood donors.
HHV-6 viremia was found only in patients with multiple sclerosis, predominantly
in the active phase of the disease. A significantly higher frequency of HHV-7
reactivation in patients with demyelinating diseases of the peripheral nervous
system suggests also its association with demyelinating processes.
======================================================
47.) [Detection of human herpesvirus type 6, human herpesvirus type 7,
cytomegalovirus and human papillomavirus in cutaneous AIDS-associated Kaposi's
sarcoma]
======================================================
Verh Dtsch Ges Pathol 1994;78:260-4
[Article in German]
Kempf W, Adams V, Hassam S, Schmid M, Moos R, Briner J, Pfaltz M.
Departement Pathologie, Universitat Zurich.
In order to evaluate a possible role of viral infections in the pathogenesis of
AIDS-associated Kaposi's sarcoma (KS), we investigated 26 cutaneous AIDS-associated
KS by polymerase chain reaction (PCR), in situ hybridization, and
immunohistochemistry. By PCR we detected human papilloma viruses (HPV),
cytomegalovirus (CMV), human herpesvirus 6 (HHV-6), and for the first time human
herpesvirus 7 (HHV-7) in the KS. The prevalence of HPV, HHV-6, and HHV-7 was
similar to or lower in KS than in normal skin tissues of AIDS patients without
KS, but higher than in normal skin of HIV-seronegative patients. All HHV-6 found
in KS were identified as HHV-6 variant B. In addition to the known HPV types 16
and 18 described in KS, we also found HPV types 6 and 33 in KS specimen. By
immunohistochemistry HHV-6 could be localized in macrophages in KS, in the
adjacent stroma as well as in normal skin of control cases. In situ
hybridization for CMV and HPV gave negative results in KS and controls.
======================================================
48.) Influenza encephalopathy associated with infection with human herpesvirus 6
and/or human herpesvirus 7.
======================================================
Clin Infect Dis 2002 Feb 15;34(4):461-6
Sugaya N, Yoshikawa T, Miura M, Ishizuka T, Kawakami C, Asano Y.
Department of Pediatrics, Nippon Kokan Hospital, Kawasaki, Kanagawa 210-0852,
Japan. [email protected]
Influenza-associated encephalopathy is often reported in young Japanese children,
but its pathogenesis is unknown. Although influenza virus can be demonstrated by
throat culture for patients with encephalopathy, cultures of samples of
cerebrospinal fluids (CSF) do not yield the virus. Eight patients with
encephalopathy or complicated febrile convulsions had influenza virus infection
diagnosed by means of culture, polymerase chain reaction (PCR), or rapid
diagnosis using throat swabs. In all 8 cases, the results of PCR testing of CSF
specimens for influenza virus were negative. On the other hand, human
herpesvirus 6 (HHV-6) DNA was demonstrated in CSF specimens obtained from 2 of 8
patients. In 3 of 8 patients, the presence of human herpesvirus 7 (HHV-7) DNA
was demonstrated in CSF specimens. Some cases of influenza-associated
encephalopathy reported in Japan may be attributable to a dual infection with
influenza virus and HHV-6, -7, or both. Another possibility is that latent HHV-6
or HHV-7 in the brain is reactivated by influenza, causing encephalopathy or
febrile convulsions.
======================================================
49.) Human herpesvirus 6 and human herpesvirus 7 infections in renal transplant
recipients and healthy adults in Turkey.
======================================================
Arch Virol 1994;136(1-2):183-90
Yalcin S, Karpuzoglu T, Suleymanlar G, Mutlu G, Mukai T, Yamamoto T, Isegawa Y,
Yamanishi K.
Department of Virology, Osaka University, Japan.
We explored the prevalence of human herpesvirus 6 (HHV-6) and human herpesvirus
7 (HHV-7) infections in 16 renal transplant recipients and 16 healthy controls
by virus isolation, serology, polymerase chain reaction (PCR) followed by dot
blot hybridization. HHV-6 variant A was isolated from one renal transplant
recipient. Seven patients (44%) and six controls (38%) had HHV-6 variant B DNA
in their peripheral blood mononuclear cells. The prevalence of HHV-7 DNA was
found to be the same in patients and controls (19%).
======================================================
50.) Detection of human herpesvirus-6 DNA in peripheral blood and saliva.
======================================================
J Med Virol 1990 Sep;32(1):73-6
Jarrett RF, Clark DA, Josephs SF, Onions DE.
Department of Veterinary Pathology, Veterinary School, Glasgow, United Kingdom.
Saliva and peripheral blood samples from 20 healthy adults were examined for the
presence of human herpesvirus-6 (HHV-6) DNA sequences using the polymerase chain
reaction. Eighteen out of 20 whole saliva samples contained detectable HHV-6
genomes. The majority of peripheral blood samples were also positive; however,
the results suggest that only a rare cell in the peripheral blood is infected.
Serological studies did not reveal any correlation between HHV-6 antibody titre
and the ability to detect HHV-6 DNA. The data indicate that HHV-6 genomes
persist in the peripheral blood and oropharynx or salivary glands of most
healthy individuals following primary infection.
======================================================
51.) Human herpesvirus-6 and human herpesvirus-7 in the bone marrow from healthy
subjects.
======================================================
Transplantation 2000 Apr 27;69(8):1722-3
Gautheret-Dejean A, Dejean O, Vastel L, Kerboull M, Aubin JT, Franti M, Agut H.
Laboratoire de Virologie GH Pitie-Salpetriere, Paris, France.
BACKGROUND: Human herpesviruses (HHVs) 6 and 7 are recently discovered
betaherpesviruses. Although HHV-6 has been associated with disordered
hematopoiesis in bone marrow transplant recipients, little information is
available on the presence of both viruses in the bone marrow from healthy
subjects. METHODS: We detected HHV-6 and HHV-7 DNA by means of polymerase chain
reaction in bone marrow and peripheral blood samples from 18 healthy subjects
who underwent total hip arthroplasty. RESULTS: Genomic HHV-6 and HHV-7 DNA were
detected in 11% and 67% of the blood samples, respectively, and in 28% and 50%
of the bone marrow samples, respectively. CONCLUSIONS: Both viruses may be
present in the bone marrow without hematopoiesis disorder and can be transmitted
through bone marrow infusion. Therefore, the causative role of these two viruses
in some bone marrow diseases cannot be inferred simply from the detection of
their genome in bone marrow by means of polymerase chain reaction.
======================================================
52.) Lymphomatoid papulosis and human herpesviruses--A PCR-based evaluation for
the presence of human herpesvirus 6, 7 and 8 related herpesviruses.
======================================================
J Cutan Pathol 2001 Jan;28(1):29-33
Kempf W, Kadin ME, Kutzner H, Lord CL, Burg G, Letvin NL, Koralnik IJ.
Department of Medicine, Beth Israel Deaconess Medical Center, Harvard Medical
School, Boston, Massachusetts, USA. [email protected]
BACKGROUND: Lymphomatoid papulosis (LyP) is a chronic, recurrent
lymphoproliferative disorder of the skin that belongs to the group of primary
cutaneous CD30-positive T-cell lymphomas. Ultrastructural and clinical features
of LyP suggest that it has a viral etiology. Human herpesviruses have been
proposed as causative cofactors for LyP because of their oncogenic potential and
their association with other lymphomas. METHODS: LyP skin lesions and a LyP-derived
cell line were examined for the presence of the recently discovered oncogenic
human herpesvirus 8 (HHV-8) and the two T-lymphotropic human herpesviruses 6 and
7 (HHV-6 and HHV-7) by nested polymerase chain reaction (PCR) using virus-specific
oligonucleotide primers. Furthermore, a recently described method involving
degenerate PCR primers was applied to detect highly conserved DNA sequences
shared by a variety of herpesviruses, especially oncogenic gamma-herpesviruses,
in an attempt to identify a yet undiscovered herpesvirus associated with LyP.
RESULTS: HHV-6 and 8 could not be found in 26 archival and 11 snap-frozen LyP
lesions and a LyP tumor cell line. HHV-7 DNA sequences were detected in 14% (5
of 37) of LyP samples. HHV-6 was found in 23% (3 of 13) and HHV-7 in 8% (1 of
13) of normal skin samples from healthy individuals, respectively. Using
degenerate PCR primers to amplify the highly conserved polymerase region of
herpesviruses, no DNA sequences related to human herpesviruses could be detected.
CONCLUSIONS: LyP is not associated with HHV-6, HHV-7 and HHV-8. In addition, the
studies using degenerate PCR primers do not indicate the presence of a
previously undescribed human herpesvirus in LyP.
======================================================
53.) Presence of human herpesvirus 6 variants A and B in saliva and peripheral
blood mononuclear cells of healthy adults.
======================================================
J Clin Microbiol 1996 Dec;34(12):3223-5
Aberle SW, Mandl CW, Kunz C, Popow-Kraupp T.
Institute of Virology, University of Vienna, Austria.
Saliva and peripheral blood mononuclear cells (PBMCs) from 44 healthy young
adults were tested for human herpesvirus 6 variants A and B (HHV-6A and -6B) DNA
by a sensitive nested PCR. HHV-6B infection was ascertained in 98% of the
subjects, and 95% were found to excrete variant B in their saliva. HHV-6A was
found in the PBMCs of 16%, but was not detected in saliva samples.
======================================================
54.) Detection of human herpesvirus 6 DNAs in samples from several body sites of
patients with exanthem subitum and their mothers by polymerase chain reaction
assay.
======================================================
J Med Virol 1995 May;46(1):52-5 Related Articles, Links
Suga S, Yazaki T, Kajita Y, Ozaki T, Asano Y.
Department of Pediatrics, Fujita Health University School of Medicine, Aichi,
Japan.
Polymerase chain reaction amplification was used to detect human herpesvirus 6 (HHV-6)
DNAs in peripheral blood mononuclear cells (MNCs), plasma, saliva, stool, and
urine from three patients with exanthem subitum and in peripheral blood MNCs,
plasma, and saliva from their mothers. HHV-6 DNAs were detected in MNCs during
and after the disease and were found in plasma only in the acute phase. The
virus DNAs were also detected in saliva after recovery from the illness and were
found persistently or intermittently in stool but not in urine samples after the
onset of the disease. In contrast, one of the three mothers excreted HHV-6 DNAs
persistently in saliva. None of the mothers had the virus DNAs in peripheral
blood MNCs and plasma nor a significant increase in antibody titers to HHV-6
after possible exposure from their children. These findings suggest systemic
replication of HHV-6 during the acute phase in patients with exanthem subitum
and persistent infection of the virus in several organs after recovery from the
disease.
======================================================
55.) Human herpesvirus-6 and human herpesvirus-7 infections in bone marrow
transplant recipients.
======================================================
J Med Virol 1997 Nov;53(3):295-305
Chan PK, Peiris JS, Yuen KY, Liang RH, Lau YL, Chen FE, Lo SK, Cheung CY, Chan
TK, Ng MH.
Department of Microbiology, University of Hong Kong, Queen Mary Hospital, Hong
Kong.
Human cytomegalovirus (HCMV), human herpesvirus-6 (HHV-6), and human herpesvirus-7
(HHV-7) DNA in peripheral blood leukocytes (PBL) of 61 bone marrow transplant
recipients was monitored weekly during the first 12 weeks post-transplantation
by a nested polymerase chain reaction (PCR). Thirty-seven (61%), 17 (28%), and
32 (53%) of patients had one or more PBL specimens positive for HCMV, HHV-6 or
HHV-7 DNA, respectively. HHV-7 DNA in PBL during the early post-transplant
period was associated with a longer time to neutrophil engraftment (mean 28.8
days vs 19.8 days; P = 0.01). In two patients who failed to engraft, HHV-6 DNA
and HHV-7 DNA was detected in plasma and PBL, respectively, early in their post-transplant
period. Patients with HCMV disease were more likely to have concurrent HHV-7 DNA
in PBL prior to onset of disease than were patients with asymptomatic HCMV
infection, suggesting that HHV-7 may be a cofactor in the progression from HCMV
infection to HCMV disease. In the 17 patients (179 specimens) in whom viral DNA
in plasma was studied (in addition to PBL), a positive result was found only in
3. In each, viral DNA in plasma appeared to correlate with clinically
significant disease. HHV-7 DNA in plasma was associated with encephalitis in an
allograft recipient.
======================================================
56.) High prevalence of HHV-6 DNA in peripheral blood mononuclear cells of
healthy individuals detected by nested-PCR.
======================================================
J Med Virol 1994 Jun;43(2):115-8
Cuende JI, Ruiz J, Civeira MP, Prieto J.
Department of Internal Medicine, University Clinic, University of Navarra,
Pamplona, Spain.
The aim of the study was the evaluation of human herpesvirus-6 (HHV-6) infection
rate and semiquantification of viremia in healthy people. Healthy blood donors
were studied. Human herpesvirus-6 IgG and IgM antibody titers were measured by
indirect immunofluorescence assay. Human herpesvirus-6 DNA amplification (nested-PCR)
was performed in peripheral blood mononuclear cells (PBMC) and in serum.
Seventeen of 50 (34 percent) individuals were positive for IgG anti-HHV-6 and
the titers ranged from 1:40 to 1:160. None of 30 individuals was positive for
IgM anti-HHV-6, suggesting no recent infection nor reactivation. Human
herpesvirus-6 DNA was detected by nested-PCR amplification in peripheral blood
mononuclear cells but not in sera. When 1 microgram DNA was amplified, HHV-6 DNA
was detected in 8 of 20 individual (40%), but in 18 of 20 (90%) when 5
micrograms DNA were amplified. It is concluded that HHV-6 is present in a high
proportion of the healthy population but in minimal amounts, and although it can
be detected in 1.4 x 10(5) PBMC, 7 x 10(5) cells are necessary to detect most
cases. No reactivation was observed in healthy people.
======================================================
57.) Clinical features and viral excretion in an infant with primary human
herpesvirus 7 infection.
======================================================
Pediatrics 1995 Feb;95(2):187-90
Asano Y, Suga S, Yoshikawa T, Yazaki T, Uchikawa T.
Department of Pediatrics, Fujita Health University School of Medicine, Aichi,
Japan.
OBJECTIVE. To find clinical features of a virologically-confirmed patient with
primary human herpesvirus 7 (HHV-7) infection and a relationship of the
excretion of viruses between HHV-7 and human herpes-virus 6 (HHV-6). PATIENT AND
METHODS. A 13-month-old boy who had a known prior history of exanthem subitum at
6 months of age developed fever for 3 days and a skin rash appeared as the fever
was resolving. The course was accompanying with nonspecific signs and symptoms
such as anorexia, irritability, mild diarrhea, palpebral edema, mild
inflammation of pharynx, and mild occipital and cervical lymphadenopathy.
Heparinized blood samples were used for isolation of HHV-6 and HHV-7 and
detection of both virus DNA sequences by a nested polymerase chain reaction (PCR)
amplification. Samples from other body sites were also tested for their DNA
sequences using the PCR. Both virus antibody activity was measured by an
indirect immunofluorescent assay or a neutralization test. RESULTS. Cultured
mononuclear cells from the patient at the acute stage of the disease produced
morphologic changes, which reacted only with the monoclonal antibody to HHV-7
but not with the antibody to HHV-6. Both viruses were not isolated from blood
obtained at the convalescent stage. An antibody response of the patient
indicated a seroconversion to HHV-7 but not to other microbial agents including
HHV-6 and Mycoplasma pneumoniae. Both virus DNA sequences were detected in
peripheral blood mononuclear cells at acute and convalescent stages. HHV-7 DNA
was excreted into saliva and transiently into stool at an early convalescent
stage followed by HHV-6 excretion into saliva. No HHV-7 and HHV-6 was excreted
into urine. CONCLUSIONS. Clinical features of a virologically confirmed patient
with primary HHV-7 infection were comparable with those of primary HHV-6
infection and HHV-7 infection may reactivate HHV-6.
==================================================================
DATA-MEDICOS/DERMAGIC-EXPRESS No 5-(119) 04/05/2.001 DR. JOSE
LAPENTA R.
===================================================================
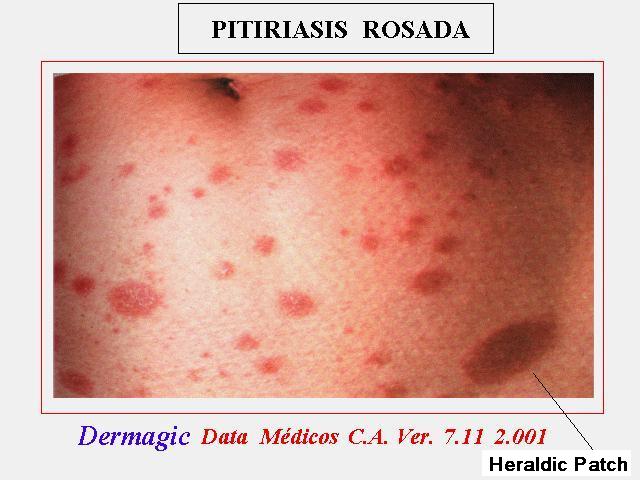
|