The Lucio's
Phenomenon. /El fenomeno de Lucio
Data-Medicos
Dermagic/Express No. 2-(94)
03 Mayo 2.000 03 May 2.000
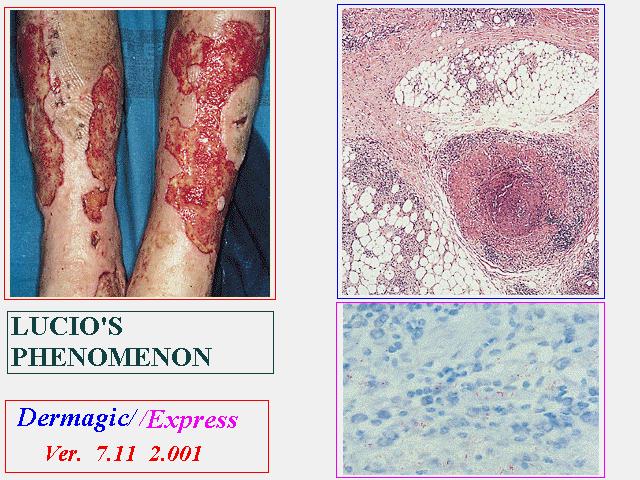
~ El fenomeno de Lucio ~
~ The Lucio's Phenomenon ~
EDITORIAL ESPANOL
=================
Hola amigos de la red. DERMAGIC de nuevo con ustedes, el tema
de hoy: EL
FENOMENO DE LUCIO. La semana pasada vi una paciente de 14 años
en mi
consulta privada, era una adolescente con una LEPRA. EL FENOMENO
DE LUCIO llamado tambien ERITEMA NECROTIZANTE es uno de los tipos
de
reaccion leprosa (Reaccion tipo II) , poco comun y descrito por
primera
vez
por Lucio y Alvarado en 1852, y reidentificado por Latapi en
1936. Se
presenta principalmente en la lepra lepromatosa difusa llamada
tambien
lepra de Lucio, caracterizada principalmente por la ausencia
de NODULOS,
este tipo de lepra es bastante comun en Centro America y Mexico.
Las
lesiones CARACTERISTICAS SON ULCERAS que afectan principalmente
miembros
inferiores, pero otras partes del cuerpo pueden estar involucradas.
Histopatologicamente se trata de una vasculitis leucocitoclastica.
El
tratamiento, TODO UN RETO. Pareciera una MENTIRA, pero HOY en
NUESTROS
DIAS
DE modernismo ENCONTRAMOS AUN ESTE FENOMENO.
Espero disfruten estas 41 referencias.
En el attach el CASO REPORTADO en la referencia No. 2
Saludos a todos !!!
Dr. Jose Lapenta R.,,,
EDITORIAL ENGLISH
=================
Hello friends of the net. DERMAGIC again with you, today's topic:
THE
LUCIO'S PHENOMENON. Last week I saw a 14 year-old patient in
my private
office, she was a adolescent with a LEPROSY. THE LUCIO'S
PHENOMENON also called ERYTHEMA NECROTIC is also one of the types
of
reaction leprous (Reaction type II), not very common and described
for
the
first time by Lucio and Alvarado in 1852, and reidentified by
Latapi in
1936. It is presented mainly in the diffuse lepromatous leprosy,
call
leprosy of Lucio, characterized mainly by the absence of NODULES,
this
leprosy type is quite
common in Central America and Mexico. The
CHARACTERISTIC lesions are ULCERS that affect mainly inferior
members,
but
other parts of the body can be involved. Histopathologically
is a
leukocytoclastic vasculitis. The treatment, an entire CHALLENGE.
It
seemed
a LIE, but TODAY in OUR DAYS OF modernism we EVEN FIND THIS PHENOMENON.
I wait you enjoy these 41 references.
In the attach file THE CASE REPORT of the REFERENCE No. 2
Greetings to ALL, !!
Dr. Jose Lapenta R.,,,
===================================================================
REFERENCIAS BIBLIOGRAFICAS / BIBLIOGRAPHICAL REFERENCES
===================================================================
1.) Lepra type reactions
2.) Diffuse Painless Ulcerations
3.) [Lucio-Latapi leprosy and the Lucio phenomenon]
4.) [Lucio's leprosy].
5.) [22 years of leprosy: histopathology]
6.) Lucio's phenomenon.
7.) Lucio's phenomenon and diffuse nonnodular lepromatous leprosy.
8.) Lucio's phenomenon: a comparative histological study.
9.) [Diffuse lepromatous leprosy disclosed by cutaneous vasculitis.
The
Lucio phenomenon].
10.) Immunologic aspects of leprosy as related to leucocytic
isoantibodies
and platelet aggregating factors.
11.) The role of protein malnutrition in the pathogenesis of
ulcerative
"Lazarine" leprosy.
12.) Dermal ultrastructure in leprosy.
13.) Lepromatous and tuberculoid leprosy: clinical presentation
and
cytokine
responses.
14.) Leprosy (Hansen's disease) in South Dakota.
15.) [Virchowian Hansen's disease, Lucio's phenomenon, cryptococcosis].
16.) Erythema nodosum leprosum in Singapore.
17.) Epidermal keratinocyte Ia expression, Langerhans cell hyperplasia
and
lymphocytic infiltration in skin lesions of leprosy.
18.) Specific antigen and antibody to Mycobacterium leprae in
the
cryoprecipitate of a patient with Lucio phenomenon.
19.) In situ characterization of T lymphocyte subsets in the
reactional
states of leprosy.
20.) Ultrastructure of the dermal microvasculature in leprosy.
21.) Lucio's phenomenon: a comparative histological study.
22.) Serum macrophage migration inhibition activity in patients
with leprosy.
23.) [Leprosy tests: diagnostic problems].
24.) Serum and tissue lysozyme in leprosy.
25.)[Reactional status of leprosy].
26.) Auricular chondritis as a rheumatologic manifestation of
Lucio's
phenomenon: clinical improvement after plasmapheresis.
27.) Contemplative immune mechanism of Lucio phenomenon and its
global
status.
28.) Plasma exchange therapy in Lucio's phenomenon.
29.) [Lepromatous leprosy with extensive ulcerations and cachexia.
The
Lucio phenomenon? Lazarine leprosy]?
30.)[2 cases of Lucio phenomenon in Paraguay].
31.) An unusual case of leprosy with pathological features common
to
Lucio's phenomenon.
32.) Primary diffuse lepromatous leprosy with erythema necrotisans
(lucio phenomenon).
33.) The "Lucio phenomenon" in diffuse leprosy.
34.) [Macular leprosy of Lucio--antimalarials in leprotic reaction].
35.) [Dermatology in the Central American tropics. I. Lucio's
spotted
leprosy. Antimalarials in the leprous reaction].
36.) [Lucio's leprosy].
37.) [Lucio phenomenon in leprosy reactions].
38.) Lucio's phenomenon: an overview.
39.) Lucio's phenomenon: an immune complex deposition syndrome
in
lepromatous leprosy.
40.) [Lucio's leprosy].
41.) Antiphospholipid antibodies thrombotic syndrome misdiagnosed
as
Lucio's phenomenon.
=============================================================
=============================================================
1.) Lepra type reactions
=============================================================
Source: Mandell, Douglas and Bennett's
Principles and Practice of Infectious Diseases Fourth Edition:
1.995
Lepra Type-1 Reactions (Downgrading and Reversal Reactions)
=========================================
Borderline leprosy patients (BT to BL) may develop before therapy
(downgrading reaction) or after the initiation of therapy (reversal
reaction) inflammation within previous skin lesions; neuritis;
at times,
new, multiple, small "satellite" maculopapular skin lesions;
and
low-grade
fever. If neuritis is not treated within the first 24 hours or
so,
irreversible nerve damage and consequent deformity and muscular
dysfunction
may result.
Reversal reactions are associated with histologic shifts toward
the
tuberculoid end of the spectrum. Lesions demonstrate increased
numbers of
CD4+ helper cells, increased levels of interferon-g and IL-2,
and an
abundance of T cells bearing g- and d-receptors. This pattern
is shared
with Mitsuda-positive skin tests and does not occur spontaneously
otherwise
in leprosy.
Lepra Type-2 Reaction (Erythema Nodosum Leprosum)
========================================
Erythema nodosum leprosum (ENL) is a syndrome affecting nearly
half of
lepromatous leprosy patients, 90 percent of the time occurring
after the
initiation of antimicrobial therapy and generally within the
first 2
years
of treatment. Clinical manifestations include, in order of frequency,
painful papules, generally on the extensor surfaces of extremities,
which
may pustulate and ulcerate and may appear as recurrent crops;
neuritis
(most frequently the ulnar nerve); fever; uveitis; lymphadenitis;
orchitis;
and glomerulonephritis. Lepromatous leprosy patients should be
forewarned
of signs and symptoms of ENL, lest their appearance result in
loss of
confidence with antimicrobial therapy and noncompliance. ENL
is
histologically an acute vasculitis or paniculitis primarily thought
to be
secondary to immune complex deposition. It is also thought to
be
associated
with a local increase in cell-mediated immunity: increased numbers
of T
helper cells and levels of IL-2 and interferon-g, and loss of
suppresor
T-cell activity. 61
Lucio's Reaction and Nerve Abscesses
============================
Patients with diffuse lepromatosis may develop shallow, often
large
polygonal sloughing ulcerations on the lower extremities that
heal
poorly,
are frequently recurrent, and may be generalized. Histopathologically,
these lesions appear to be either a variant of ENL or a result
of
arteriolar infarction. When generalized, Lucio's reaction is
frequently
fatal, generally a result of secondary bacterial infection and
sepsis.
Also, leprosy patients, particularly BT or neural leprosy patients,
may
develop nerve abscesses requiring urgent surgical decompression
and drainage.
Therapy of Reactions
================
Lepra type-1
================
reactions can be effectively treated only with corticosteroids.
We
generally initiate therapy with prednisone, 40-60 mg daily. Because
relapses commonly occur if steroids are rapidly discontinued,
steroids at
reduced doses as signs and symptoms allow must be maintained
for 2-3
months. Because of the requirement that steroids be maintained
for long
durations, strict indications are neuritis, lesions that threaten
to
ulcerate, and lesions that appear on cosmetically important places
such
as
the face.
Lepra type-2
=============
reactions (ENL) can also be effectively treated with corticosteroids,
and
short durations are often sufficient. If ENL is recurrent, thalidomide
in
a
nightly dose of 100-300 mg is the treatment of choice. In the
United
States, thalidomide cannot be prescribed to fertile women on
an
outpatient
basis and remains classified as an investigational new drug (IND)
with
investigators at the G.W. Long Hansen's Disease Center and a
number of
U.S.
Public Health Service-sponsored Regional Ambulatory Hansen's
Disease
Programs.
The mechanism of action of thalidomide for ENL is not fully understood
but
may be a result of its action to reduce IgM synthesis, 62 retard
polymorphonuclear leucocyte migration, 63 and reduce tumor necrosis
factor
(TNF) levels. 64 Other than resultant birth defects when administered
to
pregnant women in the first trimester, thalidomide is nontoxic,
its only
side effects being tranquilization, to which tolerance develops
quickly,
as
well as mild leukopenia, and constipation.
Lucio's Reaction
================
Neither thalidomide nor corticosteroid therapy has proved effective
therapy for Lucio's reaction. In severe cases, exchange transfusion
may
be
effective. In general, however, the principals of good wound
care and
appropriate antibiotics for sepsis are recommended.
=============================================================
2.) Diffuse Painless Ulcerations
=============================================================
Fernando Gallardo Hernández, MD; Jaime Notario Rosa, MD;
Anna
Jucglà Serra,
MD; Jordi Peyri Rey, MD
Ciutat Sanitària i Universitària de Bellvitge,
Barcelona, Spain
Arch Dermatol, Vol. 135 No. 8, August 1999
REPORT OF A CASE
A 62-year-old man presented with a 3-month history of severe,
ulcerating
skin lesions over the extremities. Painless violaceous macules,
livedo,
and
occasional bullae gave rise to ulcerations after a few weeks.
The lower
extremities were predominantly involved, with spontaneous amputation
of
some necrotic digits. The lesions extended proximally over the
buttocks.
The patient had a 4- to 5-year history of frequent painless traumatic
wounds that healed after 2 to 3 weeks, leaving atrophic scars.
The
patient
also noted progressive thickening of the skin, with loss of body
hair,
especially the eyebrows. Physical examination revealed a chronically
ill
man with waxy diffuse skin infiltration and a total loss of body
hair.
Numerous angular ulcerations were located over the extremities
(Figure 1)
and surrounded by a livedoid pattern. The findings of the rest
of his
examination were unremarkable except for a sensitive polyneuropathy.
Laboratory evaluation showed the following abnormal values: hemoglobin,
90
g/L; mean corpuscular volume, 67 pg; erythrocyte sedimentation
rate, 120
mm/h; and serum albumin, 16 g/L. The serum concentration of -globulin
was
increased in a polyclonal pattern. A skin biopsy specimen was
obtained
(Figure 2), and Ziehl-Neelsen staining was performed (Figure
3). (see the
attach file)
Diagnosis: Lucio phenomenon.
HISTOPATHOLOGIC FINDINGS AND CLINICAL COURSE
A punch biopsy specimen from the border of an ulcer revealed
a patchy
infiltrate of foamy histiocytes and scattered lymphocytes in
the dermis
and
subcutaneous fat, tending to be clustered around blood vessels.
Large
number of acid-fast bacilli were present in the Ziehl-Neelsen
stain of
the
specimen. Foamy histiocytes and acid-fast bacilli were also noted
in the
wall of the medium-sized arteries, with narrowing of the vessel
lumen. No
nuclear dust was observed. Slit-skin smears showed single and
clustered
acid-fast bacilli.
Multidrug therapy was initiated with 100 mg/d of oral dapsone,
50 mg/d of
clofazimine, 600 mg/d of rifampin, and a single 300-mg dose of
clofazimine
per month, with good response to date. Prednisone (40 mg) was
also
prescribed at decreasing doses for Lucio phenomenon and has been
required
for months at low doses. Our patient's ulcers healed with irregular
atrophic scars in 10 to 12 weeks.
DISCUSSION
Our patient manifested the clinical and histopathologic features
of a
diffuse, lepromatous leprosy with skin ulcerations characteristic
of
Lucio
phenomenon, a severe, necrotizing reaction described by Lucio
and
Alvarado1
in 1852. The reactional states in leprosy are characterized by
acute
inflammatory changes, and they occur more commonly toward the
borderline
and lepromatous end of the clinical spectrum. Lucio phenomenon
is an
infrequent reaction in leprosy. It has usually been described
in diffuse
lepromatous leprosy, so-called Lucio leprosy, which is unique
because of
the absence of cutaneous nodules. This type of leprosy is almost
exclusively seen in Mexico and Central America. Lucio phenomenon
is a
cutaneous necrotizing reaction that most commonly involves the
extremities
but may also affect the buttocks and trunk. The acute constitutional
symptoms of Lucio phenomenon are variable and, occasionally,
may be
fatal.2, 3 It is believed to be an immune complex–mediated disease
like the
Arthus phenomenon and is included as a type 2 reaction in leprosy.4,
5
Lucio phenomenon shows histopathologic findings of leukocytoclastic
vasculitis along with a superficial and deep mixed infiltrate
of foamy
histiocytes in a perineural and perivascular distribution. In
some
reported
cases, the vascular damage may have been the result of direct
invasion of
Mycobacterium leprae, with endothelial cell proliferation, thrombosis,
and
tissue necrosis.6
The treatment of Lucio phenomenon is the same as that for other
type 2
reactions in leprosy. Local care and supportive therapy are important
to
prevent secondary infections and loss of proteins. Prednisone
therapy,
which is initially administered at dosages of 20 to 60 mg/d and
then
tapered, may be required for weeks to months. Thalidomide (400
mg/d with
reduction to maintenance doses of 100 mg/d) may be prescribed
as an
alternative to prednisone. Clofazimine administered at a dosage
of 300
mg/d
has a useful anti-inflammatory effect. It is not necessary to
discontinue
multidrug therapy for leprosy.
REFERENCES
1. Lucio R, Alvarado Y, Latapi F, Cited by, Zamora AC, Cited by.
The
spotted leprosy of Lucio. Int J Lepr. 1948;16:421-430.
2. Pursley TV, Jacobson RR. Lucio's phenomenon. Arch Dermatol.
1980;116:
201-204. MEDLINE
3. Bernadat JP, Faucher JF, Huerre M. Lèpre lépromateuse
diffuse
révélée
par une vasculite cutanée: le phenomene de Lucio. Ann
Dermatol
Venereol.
1996;123:21-23. MEDLINE
4. Touma DJ, Phillips TJ, Kurban AK, Goldberg L. Recurrent rapidly
progressive infiltrated plaques and bullae. Arch Dermatol.
1996;132:1432-1434. MEDLINE
5. Murphy GF, Sánchez NP, Flynn TC, Sánchez JL,
Mihm MC, Soter
NA. Erythema
nodosum leprosum. J Am Acad Dermatol. 1986;14:59-69. MEDLINE
6. Rea TH, Levan NE. Lucio's phenomenon and diffuse nonnodular
lepromatous
leprosy. Arch Dermatol. 1978;114:1023-1028. MEDLINE
=============================================================
3.) [Lucio-Latapi leprosy and the Lucio phenomenon]
============================================================
ARTICLE SOURCE: Acta Leprol (Switzerland), Jul-Sep
1983, 1(3) p115-32
AUTHOR(S): Saul A; Novales J
PUBLICATION TYPE: JOURNAL ARTICLE; REVIEW (18 references)
ABSTRACT: The Lucio-Latapi's leprosy or diffuse lepromatous
leprosy is a
clinical variety of lepromatous leprosy first described by Lucio
and
Alvarado in 1852 and reidentified by Latapi in 1936. It is frequent
in
Mexico (23%) and in Costa Rica and very rare in other countries.
It is
characterized by a diffuse infiltration of all the skin which
never is
transformed into nodule, by a complete alopecia of eyebrows and
eyelashes
and body hair, by anhydrotic and dysesthesic zones of the skin
and by a
peculiar type of lepra reaction named Lucio's phenomenon or necrotic
erythema which is a vascularitis of vessels especially of the
dermohypodermic union and of the hypodermis. Clinically this
vascularitis
is represented by well-shaped erythematous spots, later becoming
necrotic
with scabs, ulcerations and scars. Three points of confusion
are
stressed:
the differences between nodules and nudosities, Lucio's leprosy
and
Lucio's
phenomenon and necrotic erythema and necrotic erythema nodosum
leprosum.
The differences between the pure and primitive form of Lucio's
leprosy
and
the secondary one is also discussed such as the laboratory findings,
histopathological data, pronostic and treatment. Lucio's leprosy
is
considered the most anergic one of the all immunological spectrum
of leprosy.
=============================================================
4.) [Lucio's leprosy].
=============================================================
Med Cutan Ibero Lat Am 1982;10(1):41-6 Related Articles, Books,
LinkOut
Gibert E, Cubria JL, Gratacos R, Castro J, Monfort J, Castel T,
Lecha M
A case of diffuse lepromatous leprosy with lepra reaction type
II-Lucio's
phenomenon-in a 24 years old male patient is reported. The histological
examination of the necrotic lesions and of the apparently normal
skin
showed the presence of dense perivascular and perianexial
lymphohystiocitic
infiltrates with great quantities of bacilli. The first biopsy
did not
show
a picture a leuccocytoclastic vasculitis but only areas of necrosis.
The
immunofluorescence studies revealed on direct examination complement
deposits on vessel walls. The complement levels in blood were
lowered and
circulating inmunecomplexes were also detected. These data confirm
the
opinion that Lucio's phenomenon is caused by circulating inmunecomplexes
fixed on dermal vessel walls causing skin necrotic lesions.
=============================================================
5.) [22 years of leprosy: histopathology]
=============================================================
AU: Dionisio-de-Cabalier-ME; Perez-HJ
AD: Ia. Catedra de Patologia, Facultad de Ciencias Medicas, Hospital
Nac,
de Clinicas, U.N.C.
SO: Rev-Fac-Cien-Med-Univ-Nac-Cordoba. 1995; 53(1): 17-21
AB: In the present study, the frequency of histopathological
reports of
leprosy carried out in the last 22 years at the Fst Chair of
Pathology
(Medical School, U. N.C) was determined. Our findings on the
frequency of
pure forms of leprosy agree with those reported by the O.M.S.
On the
contrary, that was not the case with respect to reactive forms,
since the
phenomenon of Lucio and Alvarado was more frequent in endemic
zones.
=============================================================
6.) Lucio's phenomenon.
=============================================================
ARTICLE SOURCE: Arch Dermatol (United States), Feb
1980, 116(2) p201-4
AUTHOR(S): Pursley TV; Jacobson RR
PUBLICATION TYPE: JOURNAL ARTICLE
ABSTRACT: A 38-year-old woman had diffuse, nonnodular,
lepromatous
leprosy
and Lucio's phenomenon. Most cases of Lucio's phenomenon have
been
reported
to have a leukocytoclastic vasculitis as the underlying pathologic
abnormality. In this patient, however, the histologic picture
of an early
lesion of Lucio's phenomenon showed a milk, mononuclear cell
infiltration,
endothelial swelling, vascular thrombosis, and ischemic necrosis.
Lepra
bacilli were abundant around nerves and blood vessels, and many
were
noted
in vascular walls and endothelium. Our findings raise the possibility
that
some cases of Lucio's phenomenon may be caused by vascular damage
due to
direct invasion of Mycobacterium leprae and not necessarily by
leukocytoclastic vasculitis.
=============================================================
7.) Lucio's phenomenon and diffuse nonnodular lepromatous leprosy.
=============================================================
ARTICLE SOURCE: Arch Dermatol (United States), Jul
1978, 114(7) p1023-8
AUTHOR(S): Rea TH; Levan NE
PUBLICATION TYPE: JOURNAL ARTICLE
ABSTRACT: The records of ten patients with Lucio's phenomenon
showed
clinical and histopathological changes similar to those described
by
others. Lucio's phenomenon is a syndrome distinct from erythema
nodosum
leprosum as indicated by an absence of fever, leukocytosis and
tenderness,
a failure to respond to thalidomide, and a restriction to patients
with
diffuse nonnodular lepromatous leprosy. Lymphopenia associated
with
splenomegaly in three patients and glomerulonephritis in one
patient were
unexpected findings of unknown relevance.
=============================================================
8.) Lucio's phenomenon: a comparative histological study.
=============================================================
ARTICLE SOURCE: Int J Lepr Other Mycobact Dis (United
States), Jun
1979,
47(2) p161-6
AUTHOR(S): Rea TH; Ridley DS
PUBLICATION TYPE: JOURNAL ARTICLE
ABSTRACT: To study further the pathogenesis of Lucio's
phenomenon, we
have
made a comparative histological study of 11 patients with Lucio's
phenomenon and 12 with ENL. Confirming the findings of others,
Lucio's
reaction could be distinguished from ENL by epidermal necrosis
and by
necrotizing vasculitis manifesting necrosis in the walls of superficial
vessels and severe, focal endothelial proliferation of mid-dermal
vessels.
Furthermore, in Lucio's phenomenon large numbers of AFB were
found in
evidently normal and in swollen or proliferating endothelial
cells. We
hypothesize that patients with Lucio's phenomenon have an exceptionally
deficient defense mechanism, allowing unrestricted proliferation
of AFB
in
endothelial cells, facilitating contact between bacterial antigen
and
circulating antibody and leading to infarction; also, this nadir
of
resistance allows unimpeded dissemination of AFB, accounting
for the
clinical features of diffuse non-nodular leprosy. Thus, an explanation
is
offered for the restriction of Lucio's phenomenon to patients
with
diffuse
non-nodular lepromatous leprosy.
=============================================================
9.) [Diffuse lepromatous leprosy disclosed by cutaneous vasculitis.
The
Lucio phenomenon].
=============================================================
Ann Dermatol Venereol 1996;123(1):21-3
Bernadat JP, Faucher JF, Huerre M
Clinique Paofai, Papeete, Tahiti, Polynesie francaise.
INTRODUCTION: Lucio's phenomenon, also called necrotizing erythema,
is a
rare acute manifestation which sometimes introduces diffuse lepromatous
leprosy, almost exclusively in Central American populations.
CASE REPORT:
A
76-year-old polynesian man of chinese ethnic origin had necrotizing
erythema for several months before development of Lucio's leprosy.
The
patient had necrotizing lesions of the lower limbs with large
polygonal
scars and poor general health status. Diagnosis was based on
the
discovery
of acid-fast bacilli at the pathology examination of skin biopsies.
The
necrotizing zones appeared as cutaneous vasculitis with angiogenesis
of
the
superficial dermis and presence of Hansen bacilli within the
endothelium.
DISCUSSION: This case of diffuse lepromatous leprosy, the first
reported
in
the South Pacific, emphasizes the polymorphism of leprosy and
the
importance of recognizing rare clinical forms, especially in
the tropics.
Anti-Hansen drugs are effective.
=============================================================
10.) Immunologic aspects of leprosy as related to leucocytic
isoantibodies
and platelet aggregating factors.
=============================================================
ARTICLE SOURCE: Int J Lepr Other Mycobact Dis (United
States), Jul-Sep
1975, 43(3) p239-48
AUTHOR(S): Saha K; Dutta RN; Mittal MM
PUBLICATION TYPE: JOURNAL ARTICLE
ABSTRACT: The incidences of various iso- and autoantibodies
in a random
population of 112 unselected leprosy patients is presented. Low
titers of
leucocytic isoantibodies and platelet aggregating factor were
detected in
the sera of a variable number of such patients. The leucoisoagglutinins
were found in 8% of the sera of tuberculoid as well as lepromatous
leprosy
patients, whereas the leucoisocytotoxins were detected in a larger
percentage of the lepromatous (40%) as well as tuberculoid (28%)
cases.
The
platelet aggregating factors (PAF) were positive in 51.2% and
45% of
lepromatous and tuberculoid cases respectively. Of the 21 positive
sera
for
PAF, the antiplatelet factor by antihuman globulin consumption
test could
be demonstrated only in 66.6% and 50% of lepromatous and tuberculoid
sera
respectively. To study the frequencies of these newly detected
antibodies
or antibody-like factor and to compare their occurrences with
other
well-documented autoantibodies present in the sera of leprosy
patients:
cryoglobulins, antinucleoprotein antibody and thyroglobulin
autoprecipitin
were also studied in the sera of the same population of leprosy
patients.
It has been observed that the simultaneous occurrence of all
these auto-
and isoantibodies in the serum of one patient is a rare phenomenon.
Leucocytic and platelet counts of these patients having antibodies
against
leucocytes and platelets were found to be within normal limits.
Accordingly, it is suggested that the low levels of antileucocyte
antibody
and antiplatelet factor are probably harmless to the hosts. On
the other
hand, it is postulated that these antibodies may act as enhancing
factors
by being specifically adsorbed on the lymphoid cells, thus rendering
them
unresponsive to mitogenic stimulus in vitro. From these studies
it seems
that leprosy, especially the lepromatous type, is associated
with some of
the serological features suggestive of an autoimmune aberration.
=============================================================
11.) The role of protein malnutrition in the pathogenesis of
ulcerative
"Lazarine" leprosy.
=============================================================
ARTICLE SOURCE: Int J Lepr Other Mycobact Dis (United
States), Jul-Sep
1976, 44(3) p346-58
AUTHOR(S): Skinsnes LK; Higa LH
PUBLICATION TYPE: JOURNAL ARTICLE
ABSTRACT: 1. Clinical and necropsy observations in lepromatous
leprosy
associated with severe emaciation and accompanying hypoproteinemia
suggest
that protein deprivation may be of pathogenic significance in
the
ulcerative phenomenon that is designated "Lazarine leprosy".
2. An
experimental utilizing Wiersung rats infected with Mycobacterium
lepraemurium and maintained on a protein-free diet was developed
for the
purpose of studying the effect of protein starvation on the course
of
chronic mycobacterial disease similar to lepromatous leprosy
with respect
to pathogen and host inflammatory response. 3. It was possible
to
maintain
the experimental animals on a protein-free diet for up to 18
weeks of
concomitant M. lepraemurium infection. This was long enough for
the
infection to disseminate to a degree that was evident in control
animals
only several weeks later. 4. The protein-deprived animals showed
decreased
inflammatory response to the pathogen, presented more rapid dissemination
of the infection and harbored more bacilli per macrophage than
did
animals
similarly infected but maintained on a protein adequate diet.
This
indicates impairment of native cellular immunity by protein deprivation
through decrease in ability of macrophages to inhibit bacillary
multiplication. 5. There was no evidence of impairment of macrophage
ability to phagocytose the pathogens. 6. Morphologically the
increased
dissemination of pathogens and decrease in inflammatory response
was
similar to the increase in number and extent of visceral lesions
seen in
Lazarine leprosy. Decreased ability to dispose of the infecting
bacilli
was
similar in the two models, human and animal. The animal model
does not,
as
does lepromatous leprosy, involve the skin in the infection.
Hence
comparable ulcerative phenomena were not replicated in the animals.
7. It
is suggested that Lazarine leprosy may result from enhanced lepromatous
leprous infection occurring as a result of protein malnutrition.
The
pathogenic mechanism appears to be impairment of cellular immunity
probably
enhanced by concomitant impairment of humoral antibody immunity
resulting
also in decreased resistance to pyogenic and other secondary
pathogens.
The
tissue edema attendant on decreased serum osmotic pressure due
to
lowering
of the serum protein fractions enhances the probability of ulceration.
=============================================================
12.) Dermal ultrastructure in leprosy.
=============================================================
ARTICLE SOURCE: Arch Pathol Lab Med (United States),
May 1984, 108(5)
p383-6
AUTHOR(S): Van Hale HM; Turkel SB; Rea TH
PUBLICATION TYPE: JOURNAL ARTICLE
ABSTRACT: We studied the ultrastructure of the dermal inflammatory
response in 18 patients with leprosy. Biopsy specimens from 14
lepromatous
patients, including four with Lucio's phenomenon and four with
erythema
nodosum leprosum, were compared with biopsy specimens from one
borderline
lepromatous and three borderline tuberculoid patients. In all,
the dermal
infiltrate consisted of macrophages, lymphocytes, and mast cells.
This
infiltrate was predominantly perivascular, and chronic reactive
changes
were found in the small dermal vessels. The macrophages contained
phagocytized organisms within membrane-bound vacuoles and a wide
variety
of
lysosomal residual dense bodies. Intraendothelial organisms were
occasionally seen, especially in biopsy specimens from the patients
with
Lucio's phenomenon. The greatest number of mast cells were also
seen in
the
infiltrate in those cases. The frequent close association of
macrophages
with lymphocytes and mast cells suggests an interrelationship
between
these
cells that appears typical of the host response to leprosy.
=============================================================
13.) Lepromatous and tuberculoid leprosy: clinical presentation
and
cytokine
responses.
=============================================================
Ochoa MT; Valderrama L; Ochoa A; Zea A; Escobar CE; Moreno LH;
Falabella
Dermatology Service, Universidad del Valle, Cali, Colombia.
Int J Dermatol (UNITED STATES) Nov 1996 35
(11) p786-90
OBJECTIVE: This study analyzes the major clinical characteristics
of
patients with active leprosy in relation to the in vitro immune
response
to the T-lymphocyte activator anti-CD3. METHODS: Thirty-eight
patients
with an established diagnosis of leprosy were classified according
to the
Ridley and Jopling table. Peripheral blood mononuclear
cells from both
lepromatous leprosy (LL) and tuberculoid leprosy (TL) patients
and
healthy
controls were used to evaluate lymphocyte proliferation; immunoenzymatic
assays were used to evaluate cytokine production (IL-1, IL-2,
IL-4, IL-6,
IL-10, IFN-gamma). RESULTS: Peripheral blood mononuclear
cells from both
LL and TL patients displayed blastogenic responses to anti-CD3.
The
cytokines IL-1 beta, IL-6, IL-10, and IFN-gamma were detected
in culture
supernatants. Endogenous production of IL-1 beta was significantly
higher
in cell cultures from patients with the lepromatous form of the
disease
compared to those with tuberculoid leprosy. Production
of IL-6 in
response to anti-CD3 was observed in a significantly higher proportion
of
LL than TL patients (P = 0.0025). Gamma-interferon production
did not
differ between TL and LL, but a direct correlation was observed
between
time of multidrug treatment and IFN production in vitro (P =
0.016).
Interleukin-10 was detected in culture supernatants of lymphocytes
activated by anti-CD3 from both patient groups, but not from
healthy
controls. CONCLUSIONS: The findings of this study suggest
that patients
with the two distinct forms of leprosy are capable of responding
to a
polyclonal T-lymphocyte stimulus such as anti-CD3 and provide
evidence
suggestive of alterations in the immune responses mediated by
cytokines
that may contribute to the spectrum of disease and response to
treatment.
=============================================================
14.) Leprosy (Hansen's disease) in South Dakota.
=============================================================
S D J Med 1996 Jun;49(6):185-7 Related Articles, Books, LinkOut
Burrish G, Hartmann A, Lockwood W
Department of Dermatology, Central Plains Clinic, Sioux Falls,
SD, USA.
Worldwide Hansen's disease is an important and relatively common
disease,
but is still very rare in South Dakota. Two patients are described
to
help
demonstrate the wide variety of clinical manifestations associated
with
Hansen's disease. Since the clinical appearance of Hansen's disease
is
highly variable, the following six forms of Hansen's disease
are
described:
Indeterminate, tuberculoid (TT), borderline tuberculoid (BT),
borderline
(BB), borderline lepromatous (BL), and lepromatous leprosy (LL).
In
addition, three well-recognized reactional forms of leprosy are
also
described: Type 1 (lepra reaction), type 2 (erythema nodosum
leprosum),
and
type 3 (Lucio's phenomenon). While the disease affects primarily
the skin
and nerves, health care providers of all disciplines should remain
alert
for this disease which can present with a high degree of clinical
variability.
=============================================================
15.) [Virchowian Hansen's disease, Lucio's phenomenon, cryptococcosis].
=============================================================
Hansenol Int 1988 Dec;13(2):47-56 Related Articles, Books, LinkOut
[Article in Portugese]
A 75 years old white male, for 3 years on treatment for virchowian
hanseniasis, was admitted with active HD lesions, infiltration
on the
base
of right lung, leg ulcer and malaise. After two days he developed
purpura
and hemorrhagic blisters in the limbs. The biopsy of these lesions
revealed
Lucio phenomenon. The patient worsened with mental confusion,
psychomotor
agitation and anisocoric pupils. In the 18th day of internation
the
patient
died. Necropsy revealed virchowian infiltration plenty of bacilli
in the
skin and viscera as well as tuberculoid granuloma with acid-fast
bacilli
in
the liver, spleen and bone marrow. These findings lead us to
review the
patient's classification from virchowian to borderline. In the
lungs,
leptomeninge, renal papile, prostate and thyroid it was found
loose
tuberculoid granuloma with a great amount of fungi surrounded
by a gelly
halo resembling Criptococcus neoformans. These findings and the
onset of
Lucio phenomenon are discussed in a patient that has been treated
for 3
years and still having several virchowian lesions and a great
amount of
acid-fast bacilli.
=============================================================
16.) Erythema nodosum leprosum in Singapore.
=============================================================
Ann Acad Med Singapore 1987 Oct;16(4):658-62
Giam YC, Ong BH, Tan T
Middle Road Hospital, Singapore.
Erythema Nodosum Leprosum (ENL) or Type II reaction is an immune
complex
syndrome seen in multibacillary leprosy. 20 patients with histological
confirmation of ENL in leprosy were studied from 1982 to 1986.
These
patients had a range of clinical signs, from fever, tender dusky
nodules,
bullae, ulcers to lymphadenopathy, arthralgia and neuritis. The
four
major
histological patterns are: a) classical pattern showing heavy
infiltrations
of neutrophils in three cases, b) sub-epidermal bulla pattern
with marked
oedema of the upper dermis, and collections of neutrophils in
five cases,
c) vasculitis pattern, affecting superficial and mid-dermal vessels,
leading to epidermal necrosis, bulla formation and ulceration.
Dilated
vessels, congestion, lumenal fibrin clots and fibrinoid necrosis
of
vessels
were seen, d) non-specific picture in nine cases with mild oedema,
infiltration with neutrophils, and two cases with minimal reaction
had
chronic ENL with clinical vasculitis. All the five cases with
vasculitis
showed C1q, C3 and fibrinogen in the vessels. Comparing ENL reactions
reported in Asia, our pattern is similar to that of Malaysians
with the
majority showing sub-epidermal oedema. Vasculitis is more common
in
India.
Oedema with collagen necrosis as seen in acute ENL with iritis
in New
Guinea. The Lucio's phenomenon was not seen in any of the countries
in
Asia.
=============================================================
17.) Epidermal keratinocyte Ia expression, Langerhans cell hyperplasia
and
lymphocytic infiltration in skin lesions of leprosy.
=============================================================
Clin Exp Immunol 1986 Aug;65(2):253-9 Related Articles, Books,
LinkOut
Rea TH, Shen JY, Modlin RL
Epidermal changes, Ia expression on keratinocytes, Langerhans
cell
hyperplasia and lymphocyte infiltration were sought in skin lesions
of
leprosy: 15 borderline tuberculoid (BT), six borderline lepromatous
(BL),
17 lepromatous (LL), 13 erythema nodosum leprosum (ENL), six
Lucio
reactions and nine reversal reactions. All three changes were
well
developed in BT and reversal reactions. ENL showed well developed
keratinocyte Ia and Langerhans cell hyperplasia, but little lymphocytic
infiltration. LL and Lucio tissues had some Langerhans cell hyperplasia
but
little or no keratinocyte Ia or lymphocytic infiltration. BL
tissues were
so diverse as to suggest two distinct subgroups. These findings
are
consistent with the hypothesis that keratinocyte Ia expression
is an
immunohistological sign of a cell-mediated immune (CMI) response.
However,
the Ia keratinocyte expression found in BL and ENL tissues appears
contrary
to the undifferentiated macrophages and numerous bacilli found
in the
lesions. Thus, if a sign of CMI, keratinocyte Ia expression is
not a
measure of the effectiveness of the response.
=============================================================
18.) Specific antigen and antibody to Mycobacterium leprae in
the
cryoprecipitate of a patient with Lucio phenomenon.
=============================================================
Rheumatol Int 1986;6(2):93-4 Related Articles, Books, LinkOut
Drosos AA, Brennan PJ, Elisaf MS, Stefanou SG, Papadimitriou CS,
Moutsopoulos HM
Using a sensitive and specific enzyme-linked immunosorbent assay
(ELISA)
assay we showed that the cryoglobulins of a patient with Lucio
phenomenon
contain phenolic glycolipid I antigen and a specific antibody.
=============================================================
19.) In situ characterization of T lymphocyte subsets in the
reactional
states of leprosy.
=============================================================
Clin Exp Immunol 1983 Jul;53(1):17-24 Related Articles, Books,
LinkOut
Modlin RL, Gebhard JF, Taylor CR, Rea TH
Using monoclonal antibodies and the immunoperoxidase technique,
the
numbers
and distribution of T lymphocyte subsets in the tissues of reactional
states of leprosy (six reversal reaction, nine erythema nodosum
leprosum
(ENL) and two Lucio's reaction) were determined and compared
with those
found in stable, non-reactional patients (six tuberculoid, two
borderline
lepromatous and seven lepromatous). The pattern of segregation
of the
suppressor/cytotoxic phenotype at the periphery of the granuloma
was
found
in both non-reactional tuberculoid lesions and reversal reactions,
but
was
better developed in the former. In ENL and Lucio's reaction,
as well as
in
non-reactional lepromatous tissue, the helper/inducer and
suppressor/cytotoxic phenotypes were both admixed with the aggregated
histiocytes. However, the helper/suppressor ratio in ENL (2.1
+/- 0.4)
was
significantly larger than that in non-reactional lepromatous
tissue (0.7
+/- 0.4, P less than 0.001). The immature thymocyte antigen OKT6
was
found
on scattered large non-lymphoid cells, most commonly in tuberculoid
and
reversal reaction tissues, less commonly in ENL, but only irregularly
in
non-reactional lepromatous tissue. The peripheral pattern of
the
suppressor/cytotoxic phenotype may be an immunohistological reflection
of
a
cell-mediated immune response common to both non-reactional tuberculoid
and
reversal reaction patients. The reversal of the helper/suppressor
ratio
in
ENL as compared to non-reactional lepromatous disease suggests
some role
for cell-mediated immunity in the pathogenesis of ENL. The OKT6
positive
cell is of unknown origin and function.
=============================================================
20.) Ultrastructure of the dermal microvasculature in leprosy.
=============================================================
Int J Lepr Other Mycobact Dis 1982 Jun;50(2):164-71
Turkel SB, Van Hale HM, Rea TH
Infection with M. leprae may lead to the presence of the organism
within
the dermal vascular endothelium, a phenomenon most pronounced
in
lepromatous leprosy. In order to study the ultrastructural features
of
the
dermal microvasculature in leprosy, biopsies from 18 patients
with
lepromatous (14), borderline lepromatous (1) and borderline tuberculoid
(3)
leprosy were examined. Four patients with Lucio's phenomenon
and four
with
erythema nodosum leprosum were included. The ultrastructural
changes in
the
dermal microvasculature included endothelial swelling and hypertrophy,
increased endothelial and pericytic cytoplasmic processes, and
pronounced
basal lamina reduplication. Occasional large, pale, endothelial
cells
with
widely dispersed organelles were encountered. Phagocytized,
membrane-bound
intraendothelial organisms were found, similar in appearance
to those
within dermal macrophages. The predominantly perivascular dermal
inflammatory infiltrate consisted of lymphocytes, macrophages
and mast
cells. The observed ultrastructural changes in the dermal
microvasculature
are similar to those previously described in the endoneurial
vessels.
While
reflecting nonspecific responses of the dermal microvasculature
in
chronic
inflammation, the findings support a possible role of the small
dermal
vessels in the chronic nature of the host's response to infection
with M.
leprae.
=============================================================
21.) Lucio's phenomenon: a comparative histological study.
=============================================================
Int J Lepr Other Mycobact Dis 1979 Jun;47(2):161-6
Rea TH, Ridley DS
To study further the pathogenesis of Lucio's phenomenon, we have
made a
comparative histological study of 11 patients with Lucio's phenomenon
and
12 with ENL. Confirming the findings of others, Lucio's reaction
could be
distinguished from ENL by epidermal necrosis and by necrotizing
vasculitis
manifesting necrosis in the walls of superficial vessels and
severe,
focal
endothelial proliferation of mid-dermal vessels. Furthermore,
in Lucio's
phenomenon large numbers of AFB were found in evidently normal
and in
swollen or proliferating endothelial cells. We hypothesize that
patients
with Lucio's phenomenon have an exceptionally deficient defense
mechanism,
allowing unrestricted proliferation of AFB in endothelial cells,
facilitating contact between bacterial antigen and circulating
antibody
and
leading to infarction; also, this nadir of resistance allows
unimpeded
dissemination of AFB, accounting for the clinical features of
diffuse
non-nodular leprosy. Thus, an explanation is offered for the
restriction
of
Lucio's phenomenon to patients with diffuse non-nodular lepromatous
leprosy.
=============================================================
22.) Serum macrophage migration inhibition activity in patients
with leprosy.
=============================================================
J Invest Dermatol 1982 Nov;79(5):336-9
Rea TH, Yoshida T
We have found that 26 of 54 (48%) untreated patients with leprosy
had
serum
migration inhibitory activity, and that this was present in tuberculoid,
borderline, and lepromatous forms of the disease. Patients with
active
recreational states; i.e., reversal reactions, Lucio's reaction,
or
erythema nodosum leprosum, were particularly apt to have this
inhibitory
activity. The prevalence of inhibitory activity did not vary
significantly
with treatment, dinitrochlorobenzene responsiveness, tuberculin
responsiveness, or serum lysozyme levels.
=============================================================
23.) [Leprosy tests: diagnostic problems].
=============================================================
Acta Leprol 1981 Apr-Jun;(83):11-9 Related Articles, Books, LinkOut
[Article in French]
Strobel M, Ndiaye B, Marchand JP, Stach JL, Foumoux F
Two cases of reactional leprosy leading to wrong diagnosis are
reported.
The first one concerns a reversal reaction predominantly neuritic,
initially taken for polyarthritis. The second one concerns an
erythema
nodosum leprosum with extensive cutaneous necrosis (Lucio's phenomenon
or
ulcerative lazarine leprosy). Main aspects and mechanisms of
leprosy
reactional states are reviewed. It is emphasized that errors
or delays in
diagnosis are often caused by failing to recognize cutaneous
or neuritic
symptoms.
=============================================================
24.) Serum and tissue lysozyme in leprosy.
=============================================================
Infect Immun 1977 Dec;18(3):847-56 Related Articles, Books, LinkOut
Rea TH, Taylor CR
Mean serum lysozyme values were found to be elevated in untreated
leprosy
patients. Statistically significant elevations were present in
each of
the
three major categories of leprosy, tuberculoid, borderline, and
lepromatous. Values were particularly high in patients with severe
reversal
reactions or Lucio's phenomenon. Prolonged sulfone therapy was
associated
with a fall in serum lysozyme values. With an immunoperoxidase
method to
localize lysozyme in leprous tissues, two distinct staining patterns
were
found, granular and saccular. The grandular pattern of lysozymal
staining
was found in epithelioid cells and in giant cells, and the intensity
of
staining showed a positive correlation with serum lysozyme levels.
Conversely, a saccular pattern of lysozymal staining was found
in
lepromatous histiocytes, buth the intensity of staining was unrelated
to
serum lysozyme levels; the saccular structures contained dense
aggregates
of Mycobacterium leprae. These two patterns of staining probably
represent
different functional responses of monocyte-derived granuloma
cells,
whereas
the serum levels reflect, to a varying degree, both the absolute
number
of
such cells and the rate of secretory activity of this cell population
as
a
whole.
=============================================================
25.)[Reactional status of leprosy].
=============================================================
Med Cutan Ibero Lat Am 1975;3(3):199-208 Related Articles, Books
Alonso AM
Reactional leprosy is studied according to its clinical forms
A)
Lepromatous a) Acute lepromatization: encroaching and invasive
nature;
the
patient becomes more and more lepromatous ; bad prognosis. b)
Erythema
nodosum: "contusiform dermatitis"; variable prognosis not so
bad as it is
in the preceding case; allergic nature and its evolution is usually
detained and therapeutics efficient. c) Erythema multiform. d)
Lucio's
phenomenon: vascular lesions and consequently necrosis as a complication
of
the "erythema necrotisans" (beautiful leprosy). B) Tuberculoid
Reactional
tuberculoid is the only one in this benign type, the Mitsuda's
test must
always be positive and prognosis consequently good. C) Dimorphous
or
"Borderline" whose Mitsuda's test is mostly negative, sometimes
positive,
but not stable. The lesions may stimulate the tuberculoid leprids
but
they
invade mucous membranes, are impregnated by pigmentation, may
present the
Unna's band, and other characteristics of the Lepromatous type.
Are
associated (fever, asthenia and emaciation). Prognosis not very
good,
because of the possibility of lepromatization, according to its
tendency.
Evolution slower and frequent relapses. Besides there are nodular
lesions.
Pathogeny 1) Perifocal allergic reaction (Jadassohn). Similar
to
epituberculosis and Herxheimer reaction. 2) Septicemia. Sensitized
tissues
inside or outside the lesions, are invaded by the bacilli and
so the
allergic reaction takes place. Even without culture resources,
Mycobacterium leprae has been found in the blood by direct examination.
3)
Autoimmunization (Waldenstrom, Matthews and Trantman, 1965).
Based upon
the
similarity between both humoral syndromes, in leprosy reactions
and
collagenous, diseases, as to: hypergammaglobulins, hypercryoproteins,
antigammaglobulins, serological reactions (Wassermann, Kahn,
Kline, VDRL)
positives, Antistreptolysin O, protein C reactive, antinuclear
factors,
latex and Wadler-Rose test positives (rheumatoid tests) lowering
of
complement. If leprosy reaction is like this, it should be the
less
agressive of the autoimmune diseases. a) Its eruptions are cyclic
not of
long standing duration, as a general rule. b) Its prognosis has
been
recognized as good, except lately, because of the use of corticoid
therapy
which has been fatal, in many cases. After some years the leprosy
reaction
cures spontaneously. Treatment (see article)
=============================================================
26.) Auricular chondritis as a rheumatologic manifestation of
Lucio's
phenomenon: clinical improvement after plasmapheresis.
=============================================================
Ann Intern Med 1983 Jan;98(1):49-51
Piepkorn M, Brown C, Zone J
=============================================================
=============================================================
27.) Contemplative immune mechanism of Lucio phenomenon and its
global
status.
=============================================================
J Dermatol 1987 Dec;14(6):580-5
Sehgal VN, Srivastava G, Sharma VK
=============================================================
=============================================================
28.) Plasma exchange therapy in Lucio's phenomenon.
=============================================================
Arch Dermatol 1980 Oct;116(10):1101 Related Articles, Books,
LinkOut
Wallach D, Cottenot F, Bussel A, Palangie A, Pennec J
Publication Types:
Letter
=============================================================
=============================================================
29.) [Lepromatous leprosy with extensive ulcerations and cachexia.
The
Lucio phenomenon? Lazarine leprosy]?
=============================================================
Acta Leprol 1979 Sep-Dec;(76-77):331-3
[Article in French]
Strobel M, Ndiaye B, Carayon A
=============================================================
30.)[2 cases of Lucio phenomenon in Paraguay].
=============================================================
Repura 1973 Jan-Mar;42(1):12-5
Innami S, Legiuzamon OR, Alvarenga AE
=============================================================
=============================================================
31.) An unusual case of leprosy with pathological features common
to
Lucio's phenomenon.
=============================================================
Cent Afr J Med 1971 Jun;17(6):119-22
Taube E, Ellis BP
=============================================================
=============================================================
32.) Primary diffuse lepromatous leprosy with erythema necrotisans
(lucio phenomenon).
=============================================================
Arch Dermatol 1968 May;97(5):593-4
Moschella SL
=============================================================
=============================================================
33.) The "Lucio phenomenon" in diffuse leprosy.
=============================================================
Ann Intern Med 1967 Oct;67(4):831-6
Donner RS, Shively JA
=============================================================
=============================================================
34.) [Macular leprosy of Lucio--antimalarials in leprotic reaction].
=============================================================
Dermatol Int 1965 Jul-Sep;4(3):147-50
Padilla HC
=============================================================
=============================================================
35.) [Dermatology in the Central American tropics. I. Lucio's
spotted
leprosy. Antimalarials in the leprous reaction].
=============================================================
Rev Med Hondur 1965 Jul-Sep;33(3):129-35
Corrales Padilla H
=============================================================
=============================================================
36.) [Lucio's leprosy].
=============================================================
Division de Estudios de Posgrado e Investigacion, Facultad de
Medicina,
UNAM, Mexico, D.F.
Gac Med Mex 1996 May-Jun;132(3):333-4
Quijano-Pitman F
Publication Types:
Biography
Historical article
=============================================================
=============================================================
37.) [Lucio phenomenon in leprosy reactions].
=============================================================
Nippon Rai Gakkai Zasshi 1980 Apr-Jun;49(2):113-6
Mayama A
=============================================================
=============================================================
38.) Lucio's phenomenon: an overview.
=============================================================
Lepr Rev 1979 Jun;50(2):107-12
Rea TH
=============================================================
=============================================================
39.) Lucio's phenomenon: an immune complex deposition syndrome
in
lepromatous leprosy.
=============================================================
Clin Immunol Immunopathol 1978 Feb;9(2):184-93
Quismorio FP Jr, Rea T, Chandor S, Levan N, Friou GJ
=============================================================
=============================================================
40.) [Lucio's leprosy].
=============================================================
Actas Dermosifiliogr 1976 Jan-Feb;67(1-2):31-6
Nunez Moreno A, Sotillo Gago I, Castro Romero A, Lopez Molina
M
=============================================================
===========================================================
41.) Antiphospholipid antibodies thrombotic syndrome misdiagnosed
as
Lucio's phenomenon.
=============================================================
Int J Lepr Other Mycobact Dis 1996 Sep;64(3):320-3
Bakos L, Correa CC, Bergmann L, Bonamigo RR, Muller LF
Department of Internal Medicine, Hospital de Clinicas de Porto
Alegre,
Federal University of Rio Grande do Sul, Porto Alegre, Brazil.
===================================================================
DATA-MEDICOS/DERMAGIC-EXPRESS No 2-(94) 03/05/2.000 DR.
JOSE LAPENTA R.
===================================================================
|