Nuno Craveiro Lopes M.D.
Head
of Orthopedic and Traumatologic Department
Coordinator of Pediatric Orthopedics and Limb
Reconstructive Surgery Unit
Garcia de Orta Hospital, Almada - Portugal
Any comment, suggestion or contact can be done to: [email protected]
CLINICAL CASE PRESENTATION
Treatment of femoral chronic osteomyelitis by segmental resection, proximal bone lengthening and skin traction according Ilizarov (1995)
It has been shown in many instances that, if infection must be controlled in chronic osteomyelitis, the infected portion of the bone must be radically resected, even if this means removing a segment of an essential long bone. With the Ilizarov method, it is possible to treat severe cases of chronic osteomyelitis like the following one...
This patient is a 24 yo male, who suffered a railway accident when he was 13 years of age. From the accident resulted a serious sphacelus of the distal third of the right tight, with a tangential fracture of distal femur, associated with muscle, quadriceps tendon and skin loss. He was treated by a plastic surgeon with bone shaving and several cutaneous grafts. He got a knee anchylosis and maintained a bone infection with high debit fistulae during a 5 years period. The following 7 years he maintained a low debit fistulae, that allowed him to go on with his usual way of life. In July 1994 he had an acute episode of osteomyelitis and a Pseudomonas was detected. An image of sequestrae and a osteolytic focus was observed, with distortion and changes of consistency of the distal femoral bone structure. He was treated with IV antibiotics and submitted to a surgical treatment by drainage and drilling of the femoral medullar canal. A continuous irrigation-aspiration system was installed.
|
|
|
|
|
|
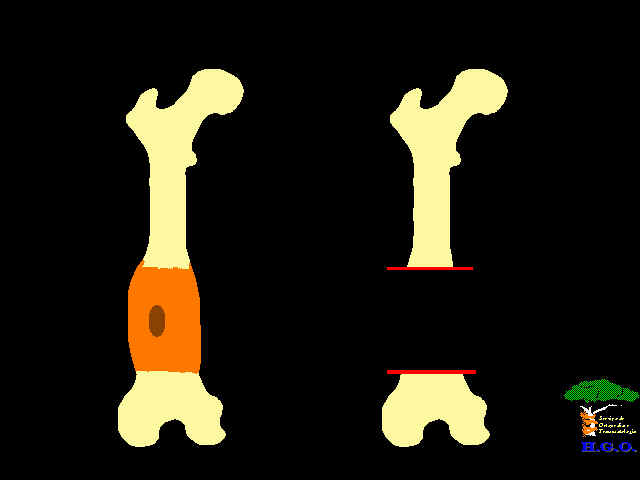
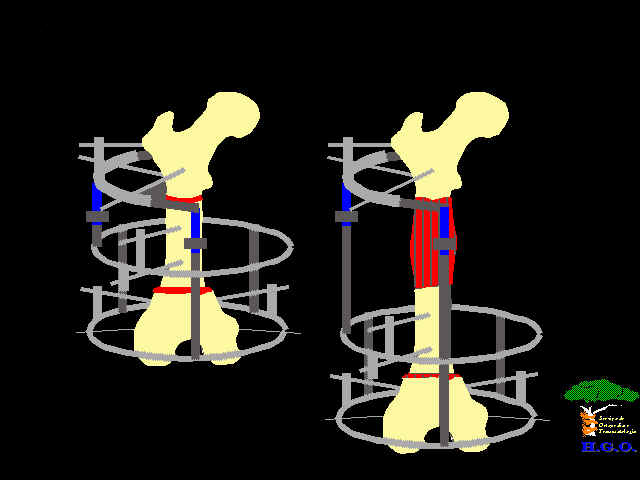
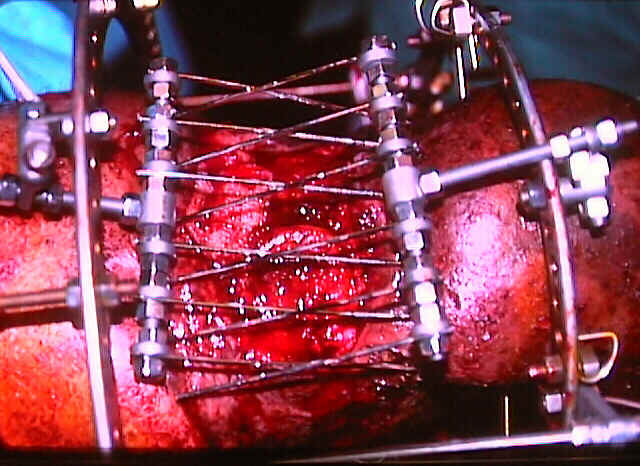
In January 1995, due to a recurrence of the infection, a 6 cm bone excision and soft tissue was done. Using the Ilizarov method, bone ends where set together with compression and a femoral proximal corticotomy with lengthening of 4.5 cm was done, to partially compensate the discrepancy and leaving a1.5cm shortening due to knee anchylosis. Simultaneously, a device was mounted for traction of the skin edges, in order to cover the skin defect. The residual granulation tissue was covered by a skin mesh graft with a good result.
|
|
|
|
|
|
|
|
|
The proximal regenerate took 5 month to mature and the excised bone ends united in a 7 months period. The past 5 years the patient has been working in building construction abroad, without any recurrence of the infection.
|
|
|