|
LIN-TELARANTA CLASSIFICATION: THE IMPORTANCE OF DIFFERENT PROCEDURES FOR DIFFERENT INDICATIONS IN SYMPATHETIC SURGERY C.-C. Lin1, T. Telaranta2 |
1 Surgical Department, Tainan Municipal Hospital, Tainan, Taiwan
2 Privatix Clinic, Tampere, Finland
ABSTRACT
Background and Aims: The second sympathetic thoracic ganglion has long been regarded as the most important structure in all sympathetic procedures for any indication, be it hand sweating, blushing, or social phobia. Earlier, we had found an interesting new basis for the selection of more specific methods in individual disorders. The aim of the present study was to either confirm the old theory or to bring forward a more appropriate theory for sympathetic surgery to be used as a classified method.
Material and Methods: Altogether 193 patients were treated in Taiwan and 55 in Finland according to the new selective principle. Endoscopic sympathetic block of the second thoracic ganglion (ESB 2) was used as a method for conflicted type of social phobia or blushing for 25 patients. ESB 3 was used for facial sweating and blushing for 55 patients. ESB 4 was used for hand and axillary sweating for 168 patients. Reflex sweating was taken as the most important sign of unsuccessful surgery.
Results: All patients benefited of the procedure in their presenting symptoms. Four of 25 cases in ESB 2 -group and three of 55 cases in ESB 3 -group had unacceptable reflex sweating. No patient with reflex sweating was found in ESB 4 -group.
These results confirm our previous findings, that sympathetic nerves innervate the human body in similar dermatome fashion as the peripheral nervous system. According to this, we organized the various sympathetic disorders into three main categories:
Conclusions: We call this new classification "Lin-Telaranta classification". Not only the incidence of complication rates is lowered but also the side effects can be predicted by the Lin-Telaranta classification in sympathetic surgery.
Key words: Endoscopic Sympathetic Block by clamping (ESB), Lin-Telaranta classification, reflex sweating, conflicted type social phobia; blushing and facial sweating; hand and underarm sweating
Endoscopic T2-sympathetic surgery (ETS2) was first used to treat Hyperhidrosis in the early twentieth century. In addition to Hyperhidrosis, indications of sympathetic surgery have expanded after the advancement of endoscopic procedure in sympathetic disorders. Some of our patients complained that the results were not what they expected. This drew our attention to an interesting assumption: is it true and appropriate that a single surgical procedure, ETS2, can treat so many different disorders?
Surgical procedures have their inherent complications. There is no doubt that "reflex sweating" is the most common postoperative complication in sympathetic surgery. Around 5 % of patients who underwent sympathetic surgery had regrets concerning post-operative reflex sweating (1, 2). Many modified sympathetic procedures, such as the micro-sympathetic procedure, highly selective sympathetic procedure, sympathetic ramus resection, partial sympathetic nerve resection or sympathetic block by clamping method (ESB) first proposed by Lin in 1996, were designed to avoid these complications, but still the results were unsatisfactory. Could it be possible that patients can both be cured from hand sweating and remain without reflex sweating after sympathetic surgery?
A common belief is that reflex sweating cannot be avoided in sympathetic surgery because other portions of the body take over the sweating of hands and face after surgery. However, many studies prove that there is no correlation between the amount of hand sweating and in the reflex sweating areas (3, 4). Moreover, reflex sweating is not found on lumbar sympathectomy for pure hyperhidrosis plantaris in our experiences. Why are there different postoperative responses between thoracic and lumbar sympathetic surgeries if the theory of "taking over the sweating" is correct?
Endoscopic Thoracic Sympathetic Block by Clamping (ESB) was invented and used to treat Hyperhidrosis for its reversibility in 1996 (5). Meanwhile another very important clinical significance was found in ESB method; that is, postoperative follow-up can be easily done by Chest X-ray to analyze which segment of the sympathetics is blocked, especially when the outcome is unexpected.
We were enlightened by two interesting cases: an 18-year-old young man, suffering from sweaty hands, with dry hands but dry face only on the right side and mild sweating on the left side after ESB2 for his sweaty hands in 1998. Chest X-ray revealed right T2 and left T3 clamped. We permuted the clamp from T2 to T3 for symmetric sweating of face, and then got an amazing result: T3 procedure could treat hand sweating and preserve various degrees of facial sweating; meanwhile, the degree of reflex sweating was decreased. After that we used ESB3 to treat hyperhidrosis.
Another interesting case was a 17-year-old young man who got dry hands after ESB3 in 1998. But he found that he had nearly normal sweating function of his face and slight sweating of his right hand in hot environment after ESB3. X-ray showed right T4 and left T3 clamped by clamps on this young man.
Several questions can be drawn:
New pathways of sympathetic innervation to human body that can explain all phenomenons in sympathetic surgery were then sought after with our series of clinical studies.
After Dr. Telaranta�s research of the relationship between the sympathetics and the limbic system of human brain, we then together classified the sympathetic disorders into three main groups according to our new findings of sympathetic nervous tracts to the human body. We call this new classification as "LinTelaranta Classification" and apply it for "different sympathetic surgical procedures to treat different sympathetic disorders".
MATERIAL AND METHODS
Endoscopic sympathetic block by clamping (ESB) is used in this study by multiple port approach under single-lumen tracheal intubation anesthesia (5, 6). The procedures of ESB are the same as conventional Endoscopic sympathetic surgery (ETS) except that Titanium clamps (Auto Suture Company, USA) are used to block, not to cut the sympathetic nervous trunk. Complete sympathetic blocking procedures are considered only when both the upper and lower ends of sympathetic ganglion are clamped.
We used different procedures to treat 248 patients with different classifications of sympathetic disorders from August 1, 2000 to February 28, 2001. ESB2, clamping upper end of T2 ganglion only, was used on 25 cases of Group I for Hyperhidrosis craniofacialis or facial blushing. ESB3 on 55 cases of Group 2 for Hyperhidrosis craniofacialis et palmaris[palm] as well as blushing. ESB4 on 168 cases of Group 3 for Hyperhidrosis palmaris and/or axillae[underarm].
RESULTS
Two of four males in Group 1 (23.5 %) regretted the surgery and asked for reversal procedures due to severe reflex sweating on their trunk within a month postoperatively. These two patients were satisfied with the results of partial recovery of facial sweating 6 months after the reversal procedure. One male in Group 2 (9.0 %) received reversal procedures for intolerable reflex sweating 6 months after ESB3. Despite dry hands after ESB4, one female in Group 3 (0.6 %) regretted the result for no simultaneous cessation of her body sweating. Without exception, moderate to severe degree of reflex sweating occurred on the trunks of Group 1 patients. Compared to Group one, less reflex sweating was found on Group 2 patients. It was very interesting that few or no reflex sweating phenomenon was found on Group 3 patients, except insignificant amounts of sweating was found on lower back or in popliteal areas only in hot environments. There were no reversal seeking patients in the Finland series.
DISCUSSION
Endoscopic thoracic sympathetic surgery (ETS) has been performed to treat more than 5500 cases of Hyperhidrosis at our hospital (Tainan Municipal hospital) since 1988. Postoperative evaluation comparing X-ray and clinical findings becomes simple and easy after ESB was unveiled in 1996. ESB opens a gate to Autonomic Nervous System (ANS) as the least atraumatic sympathetic ablation procedure today. It also provides an excellent way to study ANS because of the exact location ability of the performed block by x-ray analysis. Many bizarre and interesting postoperative conditions, so different from traditional consideration on sympathetic surgery, were and can be found in these experiments.
We have been skeptic as to how a single surgical procedure, ETS2, could treat successfully so many different sympathetic disorders, as previously stated (7). Probably many complications can be avoided if we use different surgical procedures to treat different sympathetic disorders. ETS became more accessible for surgeons after the 2nd International Symposium of Sympathetic Surgery held in Sweden. Now we should focus our research to the side effects like postoperative sweating. Many modified ETS methods have been designed for this purpose, but none of them have thus far achieved the desired result.
Even an experienced surgeon sometimes makes a mistake at the level of sympathetic ganglion in ETS. It is very difficult to evaluate the reason for unexpected results on post-ETS patients when the level of the performed surgery cannot be stated accurately. There has not been any reliable method for postoperative evaluation in sympathetic surgery until ESB was first unveiled in 1996 (5). A chest X-ray can easily confirm the clamped ganglion. ESB helped us to map the sympathetic nervous tracts and helped in reasoning the mechanism of reflex sweating.
Incidentally, we found that T3 and T4-sympathetic surgery can treat Hyperhidrosis palmaris with less postoperative complication than that of T2-sympathetic surgery. Despite the abundance of intermingling sympathetic nervous fibers in human body (8), we found, that they innervate human body by crossing up over their corresponding rib and joining the upper peripheral nerves to realize a similar dermatome distribution. Lin-Telaranta classification for
sympathetic disorders was proposed by anatomical location and by mapping new sympathetic nervous tracts, which innervate human body, to explain postoperative phenomenon in sympathetic surgery. Sympathetic disorders are thus classified into three groups:
Postoperative reflex sweating happens irrespective of cool or hot environment. In our cases, postoperative sweating happened only in hot environments which is to be considered as a normal physical response to environmental temperature. According to our new classification and new procedures, reflex sweating phenomenon happened only in Group I (none in Group 3) out of 248 cases from August 1, 2000 to February 28, 2001.
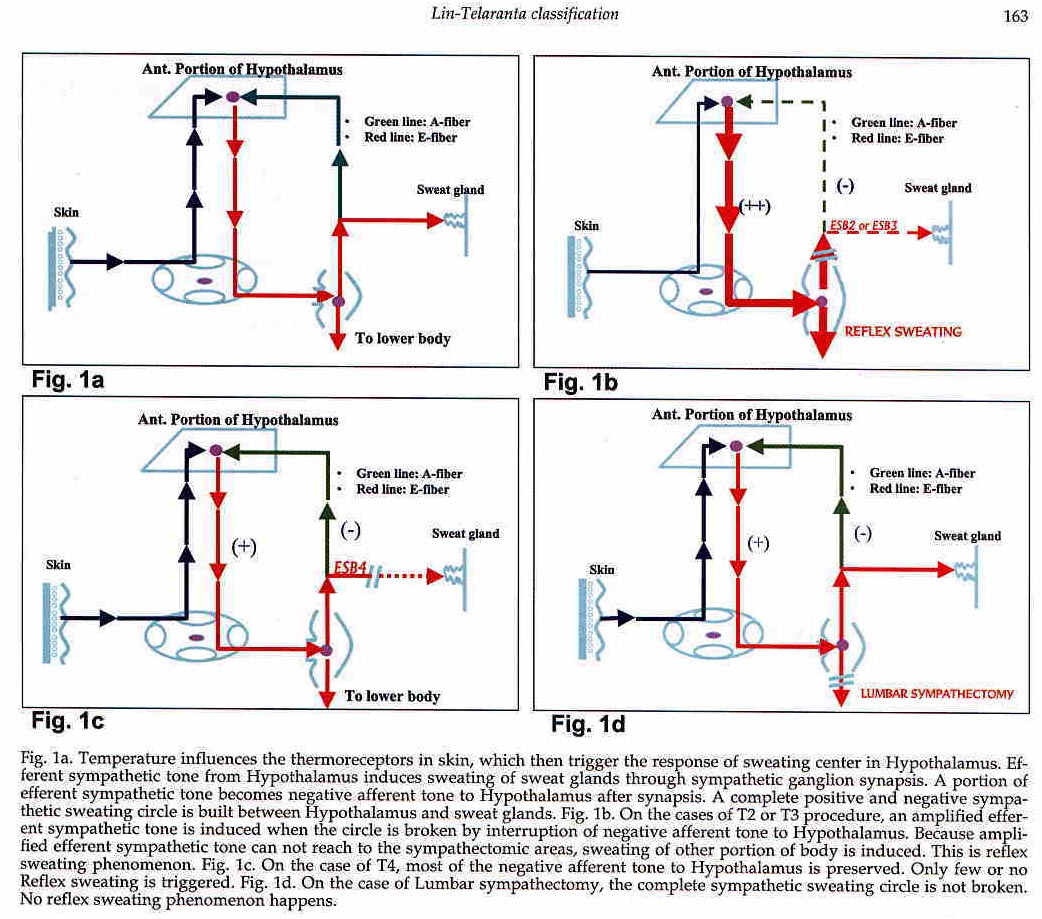
The anterior portion of Hypothalamus receives afferent thermal information from central and peripheral thermoreceptors, and releases thermoregulator efferent discharge to sweat glands (9). It is very interesting that post-sympathectomic sweating phenomenon happens not only in the cases of hyperhidrosis craniofacialis but also other sympathetic disorders in Group 1, such as facial blushing or psychic disorders (10). That coincides with the hypothesis of post-sympathectomic sweating being a reflex phenomenon regulated by a cycle of negative and/or positive feedback mechanism between body thermoreceptors, hypothalamus and sweat glands (Fig. I). Accordingly, postoperative sweating seems to be a reflex phenomenon mediated by hypothalamus, and not at all compensatory. Postoperative sweating phenomenon is not found in lumbar sympathetic surgery, because the cycle is not broken (Fig. I). Thus, we can predict that reflex sweating will not happen if we can treat hand sweating without interrupting the afferent sympathetic tone to human brain.
New sympathetic nervous tracts were mapped (Fig. 2) through our clinical experiences in different procedures for different sympathetic disorders. Sympathetic innervation to human body is roughly divided into upper and lower portions at the level of navel. The main sympathetic innervation of the upper body comes from the upper six thoracic sympathetic ganglia; while that of the lower body is from the lower six thoracic ganglia. Besides the major sympathetic innervation to their corresponding dermatome, there is multiple bifurcation of postsynaptic sympathetic nervous fibers going up and down in the sympathetic trunk that share sympathetic influence to body unequally with other segments of ganglia (11).
The upper portion of sympathetic tone has only little or no influence to lower body; while the lower portion of them have probably no influence to upper body. That is, the farther from the target organ, the less sympathetic influence is found in the respective sympathetic ganglia.
The major sympathetic innervation of the head area should be from T1 and T2 ganglia including some fibers from lower ganglions. T1 ganglion dominates in its influence to hypothalamus compared to T2 ganglion.
According to our findings, T2 and T3 influence facial sweating and blushing almost equally. Major sympathetic innervation of palmar sweat glands comes from T4 and lower ganglia. Sympathetic fibers from T3, T4 and lower should cross up and accumulate above the level of T2 ganglion to join brachial plexus before they innervate palmar sweat glands.
This is the reason why ETS2 can stop palmar as well as craniofacial sweating, then reflex sweating phenomenon is triggered simultaneously (Fig. I).
Reflex sweating will not happen if we can stop hand sweating without interrupting the afferent sympathetic tone to the human brain. We confirmed by nervous tract mapping that neither T2 nor T3; but T4 and the lower ones are the major sympathetic innervation to hands; T3 sympathetic tone is composed of only a small portion to influence the hand sweating. Major sympathetic tones at the levels above (including) T3 innervate head and neck. No nervous fiber from T2, but only a few nervous fibers from T3 innervates hands.
The fibers from T4 travel through T2 and T3 to join brachial plexus before innervating the hand. T2-sympathetic surgery blocks the sympathetic tone to both the hand and the head. This is the reason why T2-sympathetic procedures can treat hyperhidrosis palmans but with higher incidence and degree of reflex sweating. From the sympathetic nervous tract mapping, we know that ESB4 can treat hyperhidrosis palms and preserve majority of the afferent sympathetic tone to head and neck, therefore triggering no reflex sweating.