Definition and introduction
Microclbuminuria is traditionally defined as an
increase in urinary albumin too subtle to be measured by chemistry sticks for
total protein. With improved methodology, these low levels of albumin (20-200
ug/min, 30-300 mg/24h or 20-200 mg/l) can now be measured.
Microalbminuria is considered a clinically improtant indicator of
deteriorating renal funcation in diabetic and hypertensive patients. In these
patients, the microalbuminuria phase is followed by progressive incarease in
urinary protein excretion and declining glomerular filtration rate, This
results in chemistry stickpositive proteinuria, known as overt nephropathy or
macroproteinuria.
Without treatment, the patient will develop uraemia and require referral
to end-stage renal-failure programmes such as dialysis or transplantation.
Microalbuminuria has also proved to be a strong independent predictor of
atherosclerotic disease, cardiovascular mortality and overall mortality.
Increased urinary albumin excretion signals an increase in the transcapillary
escape rate of albumin and is therefore a marker of microvascular disease.
Onset of microlbuminuria (increase in urinary albumin excretion beyond
the lower limit of microalbminuria) is the most significant single predictor of
progressive microvascular disease and macrovascular disease (nephropathy,
atherosclerosis, coronary disease, retinopathy). The association of
microlbuminuria with cardiovascular disease might be explained by endothelial
dysfunction, hypertension abnormalities in lipid metabolism, insulin resistance
and protein glycosylation. THe exact mechanisms responsible for these
associations have been elucidated to some extent but many remain to be
characterised.
Pathogenesis
General
 The development of microalbuminuria probably involves
both metabolic and haemodynamic factors affecting renal microcirculation. On
the one hand, sustained hypertension is known to cause transcapillary escape of
proteins, such as albumin, by increasing the intraglomerular pressure. On the
one hand, metabolic disorders directly affect the glomerular basement membranes
and their permselectivity, thereby altering glomerular function and,
ultimately, causing golmerular sclerosis. These separate mechanisms are
differently emphasised in different diseases, which should be taken into
account in planning therapy.
The development of microalbuminuria probably involves
both metabolic and haemodynamic factors affecting renal microcirculation. On
the one hand, sustained hypertension is known to cause transcapillary escape of
proteins, such as albumin, by increasing the intraglomerular pressure. On the
one hand, metabolic disorders directly affect the glomerular basement membranes
and their permselectivity, thereby altering glomerular function and,
ultimately, causing golmerular sclerosis. These separate mechanisms are
differently emphasised in different diseases, which should be taken into
account in planning therapy.
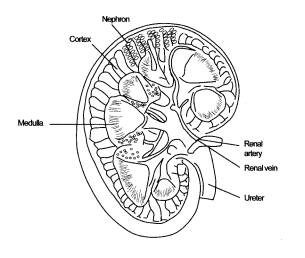
Haemodynamic aspects
Glomerular hydrostatic Pressure is normally regulated by the relative
vasoconstriction-vasodilation of the blood vessels leading to and from the
glomerulus (afferent and efferent arterioles).
Defects of this authoregulatory function may lead to increased
glomerular hydrostatic pressure and increased urinary albumin excretion or
microalbuminuria. In salt-sensitive hypertension, salt intake disturbs renal
blood flow, resulting in raised intraglomerular pressure. Indeed, salt
sensitivity is more common among groups of hypertensive patients with an
increased susceptibility to develop renal failure (black, obese, elderly and
diabetic patients).
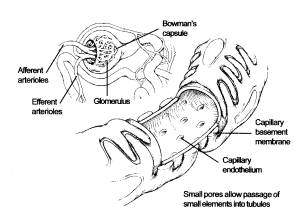
Figure2. Picture showing the glomerulus with permeable walls.
The afferent arterioles feed the blood into the Bowman's capsule to be
filtered. The glomerulus filters the blood, and the efferent arterioles
transport the filtered blood capsule to the medula. The glomerular fitrate pass
down the tubule and reaches eventually the bladder.
Metobolic aspects
As diabetes mellitus is a state chronic hyperglycaemia, it is proble
that glucose contributes to diabetic nephropathy. Urinary albumin excretion is
dependnt on both renal haemodynamics and the permselectivity of he glomerular
basement membrance. Microalbuminuria could also be due to a loss of the anionic
charge of the glomerular basement membrane. THis has been observed in diabetic
patients, in whom advanced glycosylation end neutralise the concurrent increase
in the transmembrane passage of albumin. In type 1 with the deposits of AGE
products. The risk of microalbuminuria has been found to increase with the
amount of glycosylated haemoglobin HbAc, in blood. Recent studies have also
indicated an association between microlbumin uria and impaires glomerular
charge selectivity in healthy individuals.
Metabolic syndrome
Microalbuminuria often occurs together with the metabolic syndrome
consisting of hyperinsulim aemia and insulin resistance, increased triglyceride
and decreased high-density lipoprotein (HDL) levels, hyperglycaemia for
diabetes but they have also been observed in nondiabetic and prediabetic
individuals.
THe roles of hypertension and hyperglycaemia in this context have been
discussed above, whereas the exact causal relationships between the other
factors and microalbumuminuria have not been established. It is known,
howerever, that all of these factors are independently associated with
microalbuminuria and progressive renal disease. THe metabolic syndrome as an
entity has also been albuminuria in diabeti patients.
Table 2. Charaterisation of Metabolic syndrome
Hyperinsulinanaemia
Insulin resistance
Serum triglcerides
Serum HDL cholesterol
Blood glucose
Hypertension
Clinical significance
General
The measurement of albumin excretion gives an estimate of glomerular
integrity (Including the function of tubular reabsorption). It is not clear
whether m microalbuminuria itself contributes to the deterioration of renal
function, but recent evidence suggests that it could in fact be purely a
manifestation of nephropathy. Nevertheless, microalbuminuria is a reliable
indicator of a risk of progressive renal and cardiovascular disorders. In
addition, a decrease in microalbuminuria indicates a positive response to the
chose line of therapy.
Microalbuminuria is a reliable risk indicator for renal and
cardiovascular disorders. By measuring microalbuminuria one can monitor the
patients's response to the chosen line of therapy.
Diabetes mellitus
The appearance of microalbuminuria is the first sign of nephropathy.
Patients with persistent microalbuminuria are referred to as having incipient
nephropathy. Hyperfiltrations is the first detectable alteration in renal
funcation in the course of diabetic renal disease and occurs sson after the
emergence of microalbuminuria. Urinary albumin excretion persistently exceeding
20ug min represents a 20-fold increased risk for the development of clincally
overt renal disease in patients with type 1 or 2 diabetes.
Furthermore, increased urinary albumin excretion precedes and is highly
predictive of diabetic nephropathy, end-stage renal disease and advanced
nephropathy in type 1 diabetes. Half of patients with type 1 diabetes with
overt nephropathy develop end-stage renal disease within 10 years and over
three-quarters within 20 years.
Microalbuminuria precedes and is highly predictive of diabetic
nephropathy and end-stage renal disease.
Without specific treatment,20-40% of type 2 diabetic patients with
microalbuminuria progress to overt nephropathy but only~20% developend-stage
renal disease within 20 years of the onset of overt begins to fall, the speed
of the decrease is highly variable from one individual to another, but there
may be no overall difference patients with type 2 diabetes.
In addition to being the first manifestation of nephropathy, albuminuria
is a prognostic marker for greatly increases cardivascular morbidity and
mortatlity in patients with microalbuminuria should be screened for vascular
disease and receive active therapy to reduce all cardiovascular risk factors,
including lowering of blood cholesterol. The joint occurrence of
microalbuminuria and the components of the metabolic syndrome is particularly
common among patients with type 2 albumin excretion is a strong independent
predictor of progressive renal disease, atherosclerotic disease, cardiovascular
mortality and overall mortality. Conversely insulin resistance has been
suggested to predict an elevation in urinary albumin excretion and to precede
microalbuminuria. Interestingly, approximately 20% of patients with type 2
diabetes and end-stage renal disease have a nondiabetic from of renal disease
caused by other components of the metabolic syndrome.
Albuminuria is a prognostic marker for increased cardiovascular
morbidity and mortality in patients with type 1 or 2 diabetes.
Patients with microalbuminuria should receive active therapy to reduce
all cardiovascular risk factors, including lowering of blood cholesterol.
The clinical challenge lies in identifying the high risk individuals and
developing effective measures to prevent end-stage renal disease. This is
highly relevant, as type 2 diabetes may be preventable, and good control of
blood glucose and blood pressure has been founf to prevent renal complications
in the two main types of diabetes. As mentioned above, the effectiveness of
anyrenoprotective treatment may be evaluated by monitoring the rate of urinary
albumin excretion.
Reduced proteinuria is strongly correlated with reduced progression to
end-stage renal disease.
Table 3. Stages of diabetic nephropathy.
|
Stage |
Characteristics |
|
Normoalbuminuria |
Urinary albumin excretion normal(<20ug/min) |
|
Microalbuminuria Incipient diabetic nephropathy |
Urinary albumin excretion increases (20-200 ug/min) Persistent microalbuminuria (microalbuminuria in at
least two out of three measurements within 6months) hyperfiltration, blood
pressure elevation |
|
Early overt diabetic nephropathy |
Clinical proteinuria (urinary albumin excretion>200ug/min
in two out of three measurements with in 6 months or dipstick-positive
proteinuria). Hypertension. |
|
Advanced diabetic nephropathy |
Progressive proteinuria Hypertension Declining
glomerular filtration rate (decreased creatinine clearance) |
|
End-stage renal disease |
Uraemia Nephrotic syndrome Need for renal replacement therapy (transplantation
or dialysis) |
Hypertension and cardivovascular
disease
There is an association between hypertension and albumin excretion even
in the absence of diabetes. As in diabetes, only 40% or less of patients with
essential hypertension develop microalbuminuria, and these are not necessarily
the ones with the highest blood pressure levels. Hypertensive patients who
develop microalbuminuria often have salt-sensitive hypertension, a habit of
smoking and several metabolic and haemodynamic abnormalities belonging to the
metabolic syndrome. The detection of microalbuminuria in essential hypertension
is imporatant in that it identifies a subgroup of hypertensive individulas at
higher risk of targetorgan damage. This allows measures to be undertaken fot
the prevention of complications such as hypertensive nephropathy.
Hypertensive individuals should be screened for microalbuminuria to
identify those at higher risk of target-organ damage.
Microalbuminuria has been found to be associated with cardiovascular
risk factors, cardiovascular events and mortality even in nondiabetic subjects.
The prevention and treatment of cardiovascular diseases is an adequate
management of diabetes, especially in patients with type 2 diabetes. Available
evidence suggests that although risk factors such as hypertension and hypercho
lesterolaemia are known to cause cardiovascular diseases, microalbuminuria may
in fact be a better indicator of established microvascular damage and a better
predictor of cardiovascular events. Studies have found a direct relationship
between urinary albumin excretion and fasting insulin levels, on the one hand,
and angiographic evidence of coronary artery disease, on the other. In
nondiabetic patients, microalbuminuria probably reflects not renal but more
generalished vascular damage.
In nondiabetic patients, microalbuminuria is associated with
cardiovascular risk factors and increased mortality.
Additional
implications
Pre-eclampsia in pregnancy.
The incidence of pre-eclampsia is substantially increased in diabetic
pregnancies, leading to higher maternal and perinatal morbidity and mortality.
Prepregnancy microalbuminuria has been suggested to predict pre-eclampsia in
patients with type 1 diabetes. In high-risk pregnant women without diabetes,
microalbuminuria has been found to be highly predictive of hypertensive
complications and signigicantly correlated with birth weight.
Cancer chemotherapy
Nephrotoxicity is an adverse effect of certain anticancer drugs, and
suceddful treatment of malignant disease can in fact be limited by such
toxicity. Chemotherapy-induced renal dysfunction generally involes damage to
renal vasculature or structures, heamolytic uraemic sundrome and prerenal
perfusion deficits. Microalbuminuria has been considered a senitive indicator
of glomerular damage, whereas serum cystatin C measurements appear to be a
sensitive method of detecting early reduction in glomerular filtration rate.
Microalbuminuria has been reported to be useful in detecting early glomerular
damage during cisplatin therapy. Ifosamide regimens have also been monitored
using urinary protein excretion measurements. Detection of early impairment in
renal function allows more precise adjustment of the doses of chemotherapeutic
agents.
Acute infectious nephritis
The use of tests for microalbuminuria have also been proposed for
long-term follow-up after episodes of acute infectious nephritis.
Screening,
Monitoring and treatment
Method
Screening for microalbuminuria can be performed by three methods. (1)
measurement of albumin concentration in first-void morining urine or
measurement of the albumin-to-creatinine ratio in a random spot; (2) 24-hour
urine collection with creatinine measurement, allowing simultaneous
determination of creatinine clearance; and (3) timed (e.G. 4-hours to
overnight) urine collection. THe first method is often found to be the easiest
to carry out at a doctor's office and generally provides accurate information.
Firstvoid or other morning collections are preferred because of the diurnal
variation in albumin excretion. If such timing cannot be used, it is
nevertheless important to observe uniform timing when collecting samplles from
the same individual. Specific assays are needed to detect microalbuminuria
because standard hospital laboratory assays for urinary protein are not
sufficiently sensitive. Microalbuminuria is said to be present if urinary
albumin excretion is>30mg/24h, which is equivalent to 20 ug/min or 20 mg/1
(Table 1).
Variability and interference
The rate of urinary albumin excretion depends significantly on
physiological parameters and is also rather sensitive to interfering factors.
The intraindividual variation (CV%) in urinary albumin excretion is 30-50% and
the corresponding diurnal variation (CV%) is 50-100%.
Table 4. Definitions of abnormalities in albumin excretion.
|
Category |
24-h collection (mg/24h) |
Timed collection (ug/min) |
Spot collection (ug/mg creatinine) |
|
Normal Microalbuminuria Clinical albuminuria |
<30 30-299 >300 |
<20 20-199 >200 |
<30 30-299 >300 |
Because of variability in urine albumin excretion, two of three
speciments collected within a 3-to6- month period should be abnormal
considering a patient to have crossed one of these diagnostic thresholds.
Exercise within 24h, infection, fever, congestive heart failure, marked
hyperglycemia, marked hypertension, pyuria, and hematuria may elevate urinary
albumin excretion over baseline values.
In diabetic nephropathy patients 20-50% average increases from night to
day-time in albumin excreation has been reported. Samples should not be
collected after exertion, in the presence of urinary tract infection, during
acute illness, immediately after surgery or even after an acute fluid load.
Furthermore, tubular and postrenal causes of albuminuria need to be borne in
mind Upright posture, diuresis, short-term hyperglycaemia, exercise, urinary
tract infections, marked hypertension, heart failure and acute febrile illness
can cause transient elevations in urinary albumin excretion. Tests for
microalbuminuria should be done on at least two to three occasions, two of
which should be positive to permit a diagnosis of microalbuminuria.
Diagnosis of microalbuminuria is based on two to three positive
microalbuminuria tests on different occasions.
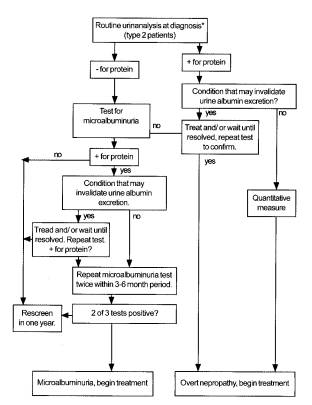
Diabetes
All patients with type 1 or type 2 diabetes should be annually screened
for microalbuminuria If a positive result for microalbuminuria is obtained in a
type 1 diabetic, the patients is obtained in a type 1 diabetic, the patient's
treatment should be intensified to diminsh urinary albumin excretion and to
half further deterioration or renal function (Figure 1).
In type 2 diabetics, microalbuminuria is a significant indicator of
increased cardiovascular risk. The level of microalbuminuria should be measured
every two to three months until a plateau is reached. The action required after
the detection of microalbuminuria in a diabetic patient consists of four
approaches, as explained below.
The level of diagnosed microalbuminuria should be measured every two to
three months.
Figure3. Screening for microalbuminuria
*In type 1 diabetes, screening for microalbuminuria should begin after 5
years disease duration.
Copyright @2001 American Diabetes Association From Diabetes Care,
Vol.25, Suppl. 1,2002 : S85_S89
Reprinted with permission from the American Diabetes Association
Actions
after deection of microalbuminuria
First, the effective management of blood glucose
concentration is fundametal. Hyperglycaemia is believed to directly damage the
glomerular basement membranes by inducing AGE product formation. According to
several major trials, retinopathic, nephropathic and possibly neuropathic
complications can be reduced by lowering blood glucose levels with intensive
therapy The UK Prospective Diabetes Study trial (UKPDS) achieved a median HbAc
of 70%, compared with a median HbAc of 7.9% with conventional therapy, and a
25% reduction in the overall microalbuminuria complication rate.
Second, hypertension should be optimally treated. The
target blood pressure for diabetic patients with microalbuminuria is
125-130/75-80 mmHg, and these demanding targets should be rigorously pursued.
The UKPDS showed that lowering bllod pressure to a mean of 144/82 mmHg significantly
reduced strokes, diabetes-related deaths, heart failure, microvascular
complications and visual loss. Angiotensin-converting enzyme (ACE) inhibitors,
which have been found to decrease urinary albumin excretrion, are currently
considered to be the first line of medication in hypertensive patients with
diabetes. According to several major trials, ACE inhibitors are effective in
not just decreasing blood pressure and proteinuria but also in slowing down the
deterioration of glomerular filtration rate in microalbuminuric and protinuric
patients. The greater antiproteinuric actio of AGE inhibitor as compared with
other antihypertensive agents appears to be due to selective vasodilation of
the offerent glomerular arterioles and a consequent decrease in intraglomerular
hydrostatic pressure. However, a direct effect of these drugs on the
permselectivity of the glomerular basement membrance cannot be ruled out. In
cases wehere a satisfactory blood pressure response is not obtained by an AGE
inhibitor alone, Diuretics and / or calcium channel blockers amy be added to
the therapeutic regimen.
Thired, the patient should be encouraged to give up smoking.
Smoking carries an additional independent risk of both diabetic and nondiabetic
progressive renal disease, as well as worsening patients' prognosis. Smoking is
also associated with an increased risk of microalbuminuric and doubling of the
rate of progression to end-stage renal disease, whereas stopping smoking has
been reported to reverse these processes.
Foutth, the intake of dietary protein should be restricted
because such a dietary modification appears to significantly decrease urinary
albumin excretion in type 1 diabetes and to slow the rate of decline of renal
function. THis is best achieved in co-operation with a nutritionist.
Table 5. Summary of actions after detection of microalbuminuria.
|
Measures to halt the progression of
microalbuminuric |
Target |
|
1. Effective control of gluvose matabolism |
|
|
2. Effective treatment of hypertensionwith ACE
inhibitors and, as reguires with diuretics and calvium vhannel blockers |
Bllod pressure target 125-130/75-80mmHg |
|
3. Stopping smoking |
|
|
4. Intake of dietary protein should be restricted |
|
Hypertension
The detection of microalbuminuric in essential hypertension is important
in that it identifies a subgroup of
hypertensive individuals at higher risk of target-organ damage. These patients
typically have several proven and modifiable risk factors for vascular and
metabolic complications, such as obesity, hyperlipidaemia and glucose
introlerance. Therefore, efforts should be aimed at treating the primary
disease as effectively as possible (target blood pressure 130/180mmHg).
Research evidence makers ACE inhibitors the first line of medication in this
context. ACE inhibitors have been demonstrated to significantly reduce
progression from macroproteinuria to overt proteinuria and from nephropathy to
end-stage renal disease even in patients without diabetes. They have also been
shown to reduce the risk for cardiovascular events without increasing
diabetes-related adverse effects (c.f. the unfavourable effects of calcium
channel blockers and beta blockers on glycaemic control.
Correction of the other above-mentioned abnormalities by lifestlye
modification and/or pharmacological means, together with the management of
blood pressure, is effective in reducing the incidence of nephropathy, diabetes
and cardiovascular disease.
Patients with hypertension and macroproteinuria should aim for pressure
levels of 130/80 mmHg.
ACE inhibitors significantly reduce progression from macroproteinuria to
evert proteinuria. Reduction in urinary albumin excretion has been conclusively
associated with improved prognosis regarding development of nephropathy and
other micro-and macrovascular complication.
In contrast to diabetes, there are so far no exact guidelines on the
course of action in the case of macroproteinuria in nodiabetic hypertension. It
has yet to be established whether correction of macroproteinuria as such
affords further protection against cardiorenal complications. Nonetheless,
macroproteinuria should alert the physician to search for other risk factors
and use effective therapies to reduce the chances of those risks resulting in
clinical manifestations.
Economic aspects
Nearly 33% of patients with diabetes mellitus develop renal
complications, including end-stagedevelop renal failure. in the United States,
diabetic kidney disease is the most common cause of end-stage renal failure.
These patients may require dialysis or renal transplantation, both of which are
expensive and may signigicantly impair the patient's quality of life. The cost
of screening for macroproteinuria has been calculated to be $2.06 billion per
year. In contrast, the cost of treating diabetic patients for renal disorders substantially
exceeds this amount ($3.4 billion per year). Evaluating diabetic paients for
macroproteinuria produces substantial cost benefits in addition to the obvious
benefits to patients in preventing this common complication of diabetes.
It is cost-beneficial to screen diabetics for macroproteinuria.
Conclusion
Tests for macroproteinuria may be considered some of the most practial,
effective and inexpensive tools for managing diabetes and hypertension in
general practice. In diabetic patients, macroproteinuria teste should be used
in parallel with HbA1c measurements to optimise the monitoring and treatment of
the disease. In hypertensive patients, with or without diabetes,
macroproteinuria testing should be used to detect patients at increased, risk for
physician to the probability of additional risk factors and to monitor the
efficacy of treatment. In a wider context, the onset and ectent of
macroproteinuria may be used for early detection of subclinical deterioration
of renal function and as an indicator of incipient progressive renal disease.
Early detection of renal impairment allows the physician to implement more
effective renoprotective strategies. It is improtant to realise that control of
macroproteinuria invariably reduces the likehood of developing end-stage renal
disease.