|
Branch Retinal Vein Occlusion
|
Early Experience PRP
|
|
-
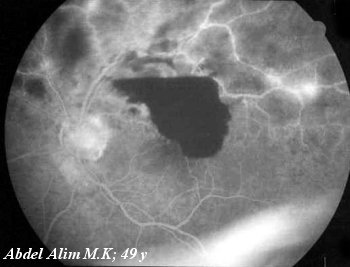
Areas of Block fluorescence corresponding to hges
-
Areas of hypofluorescence corresponding to areas of capillary non perfusion
-
Areas of hyperfuorescence corresponding to leakage from affected vascular
tree
|
-
Areas of Block fluorescence corresponding to hges
-
Tortuous dilated Lower temporal vein
|
Clinically:
-
Sudden painless recurrent attacks of blurred vision
-
Sudden painless recurrent attacks of visual field
defects
-
Sudden painless deterioration of vision due to:
-
Macular Haemorrhage
-
Macular Oedema
-
Macular Non Perfusion
-
Subhyaloid haemorrhage
-
Vitreous haemorrhage
Back
Ophthalmoscopy:
-
Segmental intra Retinal Haemorrhages in one or two quadrants according
to site of occlusion
-
Prominent venous dilatation and tortousity along the affected vessels
-
Areas of retinal oedema along the affected vessel
Back
Prognosis
-
Nearly complete resolution within one year unless complications occur.
-
Absorption of Retinal Haemorrhages within "3-18 month"
Back
Fluorescein
Angiography Evaluation:
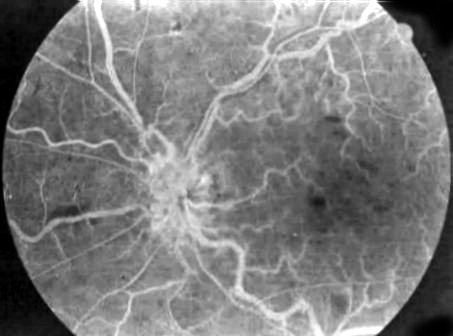
FFA demonstrates:
Segmental distribution of Retinal Vascular Abnormalities
including:
-
Areas of Block Fluorescence corresponding to areas
of Haemorrhages
-
Areas of Hypofluorescence corresponding to areas of
Capillary Non Perfusion
-
Areas of hyperfuorescence corresponding to areas
of micro aneurysms
-
Areas of collateral vessel formation
-
Areas of NVD & NVE
So the value of FFA is Evaluation
of
-
Macular Oedema with cystoid changes
-
State of Retinal Perfusion. It is of very important
prognostic and therapeutic value.
Back
Management:
Follow up for "3-4 month" till retinal/ Subhyaloid/Vitreous
haemorrhages absorb
Re Evaluate the condition:
Visual Acuity
|
Improves
|
Drops or vision does
not improve > 6/12 with best correction
|
Keep Follow up
NVD / NVE
Neovascular Glaucoma "Gonio examination without dilatation" |
Evaluate the aetiology
FFA
|
Persistent Macular Oedema with Cystoid
Formation
|
Capillary Non Perfusion involving FAZ
|
|
Grid Photo Coagulation
|
Nothing help
|
Follow "3-4 m" FFA to evaluate state of macula
|
oedema Improves
|
oedema persists
|
|
Keep Follow
|
Retreat Grid
|
|
|
Area Of capillary Non
Perfusion > 5 DD
Start PRP to avoid Neovascular Glaucoma
|
Keep Follow for:
NVD / NVE
Neovascular Glaucoma "Gonio examination without dilatation"
Prophylactic Mild Scatter PRP may and may
not be
Better Follow/4m or apply if NVD or NVE appears |
|
Back
Grid
Photocoagulation For Macular Oedema In Branch Vein Occlusion:
Argon Laser :
Spot size:
100 um
Duration:
100 msec
Power : Sufficient
to produce minimum bleach
Roles:
-
Two rows land marking temporal edge of Macula "Capillary Free Zone -
Never approximate more"
-
Extend all over but not > the vascular arcades
-
Repeated/Week staged settings = Single setting
Prophylactic Mild Scatter PRP In BVO:
-
If area of capillary non perfusion > 5DD
-
If NVD or NVE appear during per month follow up
Back
This
page
is designed
by Ahmed
Badawy
©
Copy
Right
Protected